

Effects of Testing and Disclosing Ancestry-Specific Genetic Risk for Kidney Failure on Patients and Health Care Professionals: A Randomized Clinical Trial
- PMID: 35244702
- PMCID: PMC8897752
- DOI: 10.1001/jamanetworkopen.2022.1048
Effects of Testing and Disclosing Ancestry-Specific Genetic Risk for Kidney Failure on Patients and Health Care Professionals: A Randomized Clinical Trial
Abstract
Importance: Risk variants in the apolipoprotein L1 (APOL1 [OMIM 603743]) gene on chromosome 22 are common in individuals of West African ancestry and confer increased risk of kidney failure for people with African ancestry and hypertension. Whether disclosing APOL1 genetic testing results to patients of African ancestry and their clinicians affects blood pressure, kidney disease screening, or patient behaviors is unknown.
Objective: To determine the effects of testing and disclosing APOL1 genetic results to patients of African ancestry with hypertension and their clinicians.
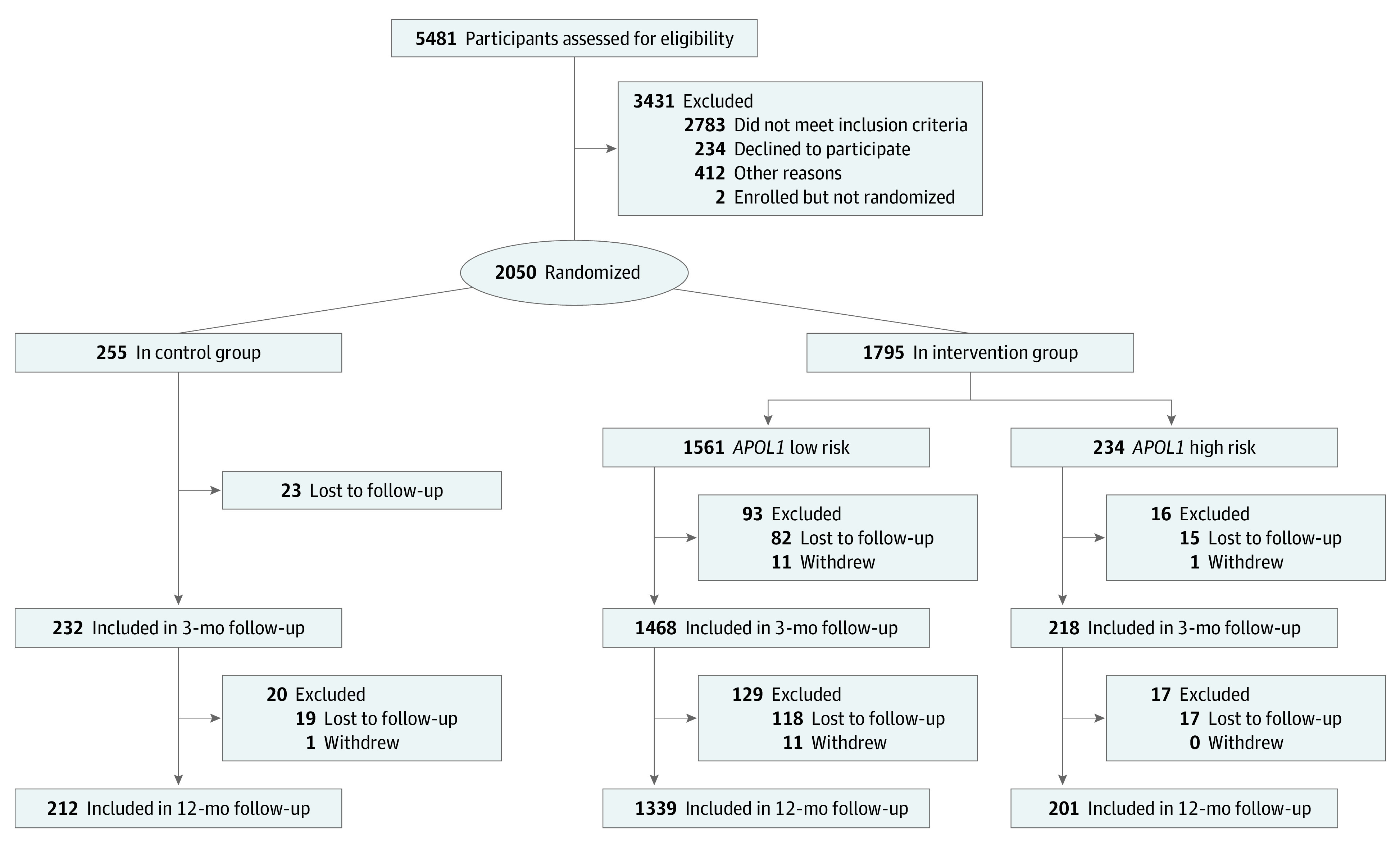
Design, setting, and participants: This pragmatic randomized clinical trial randomly assigned 2050 adults of African ancestry with hypertension and without existing chronic kidney disease in 2 US health care systems from November 1, 2014, through November 28, 2016; the final date of follow-up was January 16, 2018. Patients were randomly assigned to undergo immediate (intervention) or delayed (waiting list control group) APOL1 testing in a 7:1 ratio. Statistical analysis was performed from May 1, 2018, to July 31, 2020.
Interventions: Patients randomly assigned to the intervention group received APOL1 genetic testing results from trained staff; their clinicians received results through clinical decision support in electronic health records. Waiting list control patients received the results after their 12-month follow-up visit.
Main outcomes and measures: Coprimary outcomes were the change in 3-month systolic blood pressure and 12-month urine kidney disease screening comparing intervention patients with high-risk APOL1 genotypes and those with low-risk APOL1 genotypes. Secondary outcomes compared these outcomes between intervention group patients with high-risk APOL1 genotypes and controls. Exploratory analyses included psychobehavioral factors.
Results: Among 2050 randomly assigned patients (1360 women [66%]; mean [SD] age, 53 [10] years), the baseline mean (SD) systolic blood pressure was significantly higher in patients with high-risk APOL1 genotypes vs those with low-risk APOL1 genotypes and controls (137 [21] vs 134 [19] vs 133 [19] mm Hg; P = .003 for high-risk vs low-risk APOL1 genotypes; P = .001 for high-risk APOL1 genotypes vs controls). At 3 months, the mean (SD) change in systolic blood pressure was significantly greater in patients with high-risk APOL1 genotypes vs those with low-risk APOL1 genotypes (6 [18] vs 3 [18] mm Hg; P = .004) and controls (6 [18] vs 3 [19] mm Hg; P = .01). At 12 months, there was a 12% increase in urine kidney disease testing among patients with high-risk APOL1 genotypes (from 39 of 234 [17%] to 68 of 234 [29%]) vs a 6% increase among those with low-risk APOL1 genotypes (from 278 of 1561 [18%] to 377 of 1561 [24%]; P = .10) and a 7% increase among controls (from 33 of 255 [13%] to 50 of 255 [20%]; P = .01). In response to testing, patients with high-risk APOL1 genotypes reported more changes in lifestyle (a subjective measure that included better dietary and exercise habits; 129 of 218 [59%] vs 547 of 1468 [37%]; P < .001) and increased blood pressure medication use (21 of 218 [10%] vs 68 of 1468 [5%]; P = .005) vs those with low-risk APOL1 genotypes; 1631 of 1686 (97%) declared they would get tested again.
Conclusions and relevance: In this randomized clinical trial, disclosing APOL1 genetic testing results to patients of African ancestry with hypertension and their clinicians was associated with a greater reduction in systolic blood pressure, increased kidney disease screening, and positive self-reported behavior changes in those with high-risk genotypes.
Trial registration: ClinicalTrials.gov Identifier: NCT02234063.
Conflict of interest statement
Figures
Comment in
-
Race, Ancestry, and Genetic Risk for Kidney Failure.Am J Kidney Dis. 2022 Dec;80(6):801-804. doi: 10.1053/j.ajkd.2022.08.008. Epub 2022 Sep 12. Am J Kidney Dis. 2022. PMID: 36100174 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
