

Patient Harm and Institutional Avoidability of Out-of-Hours Discharge From Intensive Care: An Analysis Using Mixed Methods
- PMID: 35245235
- PMCID: PMC9197137
- DOI: 10.1097/CCM.0000000000005514
Patient Harm and Institutional Avoidability of Out-of-Hours Discharge From Intensive Care: An Analysis Using Mixed Methods
Abstract
Objectives: Out-of-hours discharge from ICU to the ward is associated with increased in-hospital mortality and ICU readmission. Little is known about why this occurs. We map the discharge process and describe the consequences of out-of-hours discharge to inform practice changes to reduce the impact of discharge at night.
Design: This study was part of the REcovery FoLlowing intensive CarE Treatment mixed methods study. We defined out-of-hours discharge as 16:00 to 07:59 hours. We undertook 20 in-depth case record reviews where in-hospital death after ICU discharge had been judged "probably avoidable" in previous retrospective structured judgment reviews, and 20 where patients survived. We conducted semistructured interviews with 55 patients, family members, and staff with experience of ICU discharge processes. These, along with a stakeholder focus group, informed ICU discharge process mapping using the human factors-based functional analysis resonance method.
Setting: Three U.K. National Health Service hospitals, chosen to represent different hospital settings.
Subjects: Patients discharged from ICU, their families, and staff involved in their care.
Interventions: None.
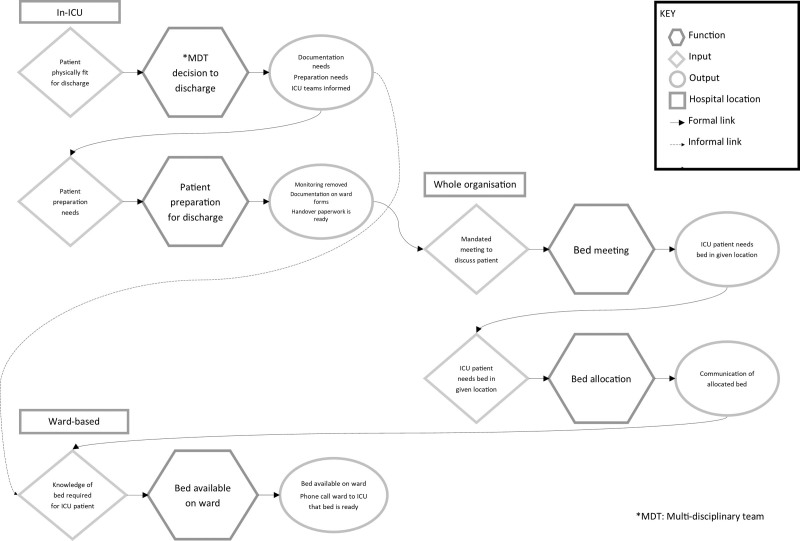
Measurements and main results: Out-of-hours discharge was common. Patients and staff described out-of-hours discharge as unsafe due to a reduction in staffing and skill mix at night. Patients discharged out-of-hours were commonly discharged prematurely, had inadequate handover, were physiologically unstable, and did not have deterioration recognized or escalated appropriately. We identified five interdependent function keys to facilitating timely ICU discharge: multidisciplinary team decision for discharge, patient prepared for discharge, bed meeting, bed manager allocation of beds, and ward bed made available.
Conclusions: We identified significant limitations in out-of-hours care provision following overnight discharge from ICU. Transfer to the ward before 16:00 should be facilitated where possible. Our work highlights changes to help make day time discharge more likely. Where discharge after 16:00 is unavoidable, support systems should be implemented to ensure the safety of patients discharged from ICU at night.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine and Wolters Kluwer Health, Inc.
Conflict of interest statement
Dr. Vollam’s institution received funding from the National Institutes of Health Research (NIHR) U.K. Research for Patient Benefit grant and the NIHR Oxford Biomedical Research Centre. Drs. Morgan’s and Watkinson’s institutions received funding from the NIHR. Dr. Pattison received support for article research from the NIHR. Dr. Watkinson’s institution received funding from Wellcome and Sensyne Health; he disclosed that he previously worked for Sensyne Health as Chief Medical Officer and holds shares in the company. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
Leveraging Robust Mixed Methodologies to Advance Implementation Research and Practice.Crit Care Med. 2022 Jul 1;50(7):1159-1161. doi: 10.1097/CCM.0000000000005551. Epub 2022 Jun 13. Crit Care Med. 2022. PMID: 35726982 No abstract available.
Similar articles
-
Problems in care and avoidability of death after discharge from intensive care: a multi-centre retrospective case record review study.Crit Care. 2021 Jan 6;25(1):10. doi: 10.1186/s13054-020-03420-5. Crit Care. 2021. PMID: 33407702 Free PMC article.
-
Surgical intensive care - current and future challenges?Qatar Med J. 2020 Jan 13;2019(2):3. doi: 10.5339/qmj.2019.qccc.3. eCollection 2019. Qatar Med J. 2020. PMID: 31976309 Free PMC article.
-
Impact of intensive care unit discharge time on patient outcome.Crit Care Med. 2006 Dec;34(12):2946-51. doi: 10.1097/01.CCM.0000247721.97008.6F. Crit Care Med. 2006. PMID: 17075364
-
Medication-related interventions to improve medication safety and patient outcomes on transition from adult intensive care settings: a systematic review and meta-analysis.BMJ Qual Saf. 2022 Aug;31(8):609-622. doi: 10.1136/bmjqs-2021-013760. Epub 2022 Jan 18. BMJ Qual Saf. 2022. PMID: 35042765 Free PMC article.
-
Healthcare stakeholders' perceptions and experiences of factors affecting the implementation of critical care telemedicine (CCT): qualitative evidence synthesis.Cochrane Database Syst Rev. 2021 Feb 18;2(2):CD012876. doi: 10.1002/14651858.CD012876.pub2. Cochrane Database Syst Rev. 2021. PMID: 33599282 Free PMC article.
Cited by
-
Ethical considerations in evaluating discharge readiness from the intensive care unit.Nurs Ethics. 2024 Aug;31(5):896-906. doi: 10.1177/09697330231212338. Epub 2023 Nov 11. Nurs Ethics. 2024. PMID: 37950598 Free PMC article.
-
A scoping review of work patterns of junior medical officer tasks in hospital out of hours.Intern Med J. 2025 Jun;55(6):968-974. doi: 10.1111/imj.70055. Epub 2025 Apr 12. Intern Med J. 2025. PMID: 40219841 Free PMC article.
-
Incidence, risk and impact of ICU readmission on patient outcomes and resource utilisation in tertiary level ICUs in Nepal: A cohort study.Wellcome Open Res. 2025 Feb 24;7:272. doi: 10.12688/wellcomeopenres.18381.3. eCollection 2022. Wellcome Open Res. 2025. PMID: 40170883 Free PMC article.
References
-
- Goldfrad C, Rowan K: Consequences of discharges from intensive care at night. Lancet. 2000; 355:1138–1142 - PubMed
-
- Pilcher DV, Duke GJ, George C, et al. : After-hours discharge from intensive care increases the risk of readmission and death. Anaesth Intensive Care. 2007; 35:477–485 - PubMed
-
- Santamaria JD, Duke GJ, Pilcher DV, et al. ; Discharge and Readmission Evaluation (DARE) Study: The timing of discharge from the intensive care unit and subsequent mortality. A prospective, multicenter study. Am J Respir Crit Care Med. 2015; 191:1033–1039 - PubMed
-
- Beck DH, McQuillan P, Smith GB: Waiting for the break of dawn? The effects of discharge time, discharge TISS scores and discharge facility on hospital mortality after intensive care. Intensive Care Med. 2002; 28:1287–1293 - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
