

A retrospective validation of CanAssist Breast in European early-stage breast cancer patient cohort
- PMID: 35245746
- PMCID: PMC8892025
- DOI: 10.1016/j.breast.2022.02.010
A retrospective validation of CanAssist Breast in European early-stage breast cancer patient cohort
Abstract
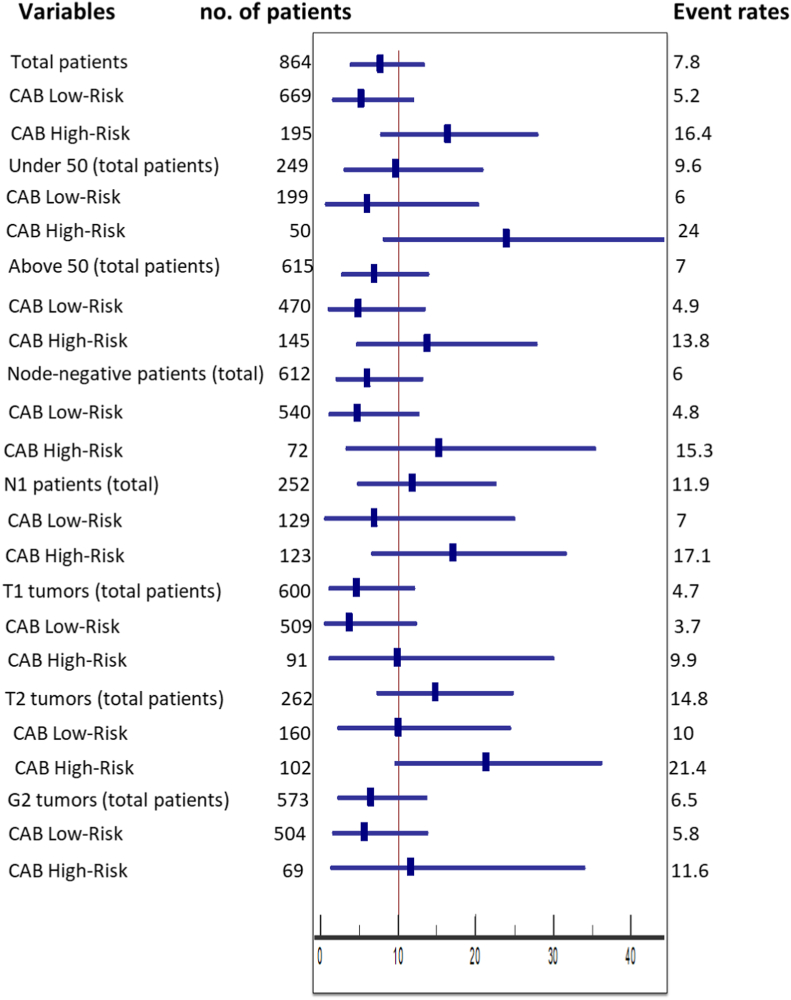
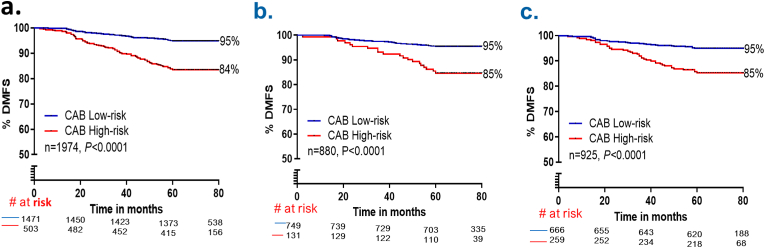
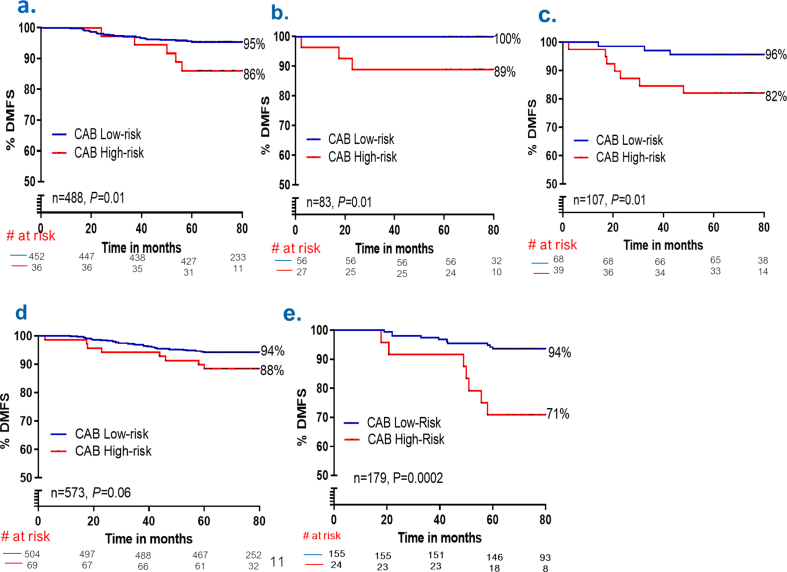
CanAssist Breast (CAB), a prognostic test uses immunohistochemistry (IHC) approach coupled with artificial intelligence-based machine learning algorithm for prognosis of early-stage hormone-receptor positive, HER2/neu negative breast cancer patients. It was developed and validated in an Indian cohort. Here we report the first blinded validation of CAB in a multi-country European patient cohort. FFPE tumor samples from 864 patients were obtained from-Spain, Italy, Austria, and Germany. IHC was performed on these samples, followed by recurrence risk score prediction. The outcomes were obtained from medical records. The performance of CAB was analyzed by hazard ratios (HR) and Kaplan Meier curves. CAB stratified European cohort (n = 864) into distinct low- and high-risk groups for recurrence (P < 0.0001) with HR of 3.32 (1.85-5.93) like that of mixed (India, USA, and Europe) (n = 1974), 3.43 (2.34-4.93) and Indian cohort (n = 925), 3.09 (1.83-5.21). CAB provided significant prognostic information (P < 0.0001) in women aged ≤ 50 (HR: 4.42 (1.58-12.3), P < 0.0001) and >50 years (HR: 2.93 (1.44-5.96), P = 0.0002). CAB had an HR of 2.57 (1.26-5.26), P = 0.01) in women with N1 disease. CAB stratified significantly higher proportions (77%) as low-risk over IHC4 (55%) (P < 0.0001). Additionally, 82% of IHC4 intermediate-risk patients were stratified as low-risk by CAB. Accurate risk stratification of European patients by CAB coupled with its similar performance inIndian patients shows that CAB is robust and functions independent of ethnic differences. CAB can potentially prevent overtreatment in a greater number of patients compared to IHC4 demonstrating its usefulness for adjuvant systemic therapy planning in European breast cancer patients.
Keywords: CanAssist Breast; European; Hormone-receptor positive; Prognostication; chemotherapy; early-stage breast cancer; recurrence.
Copyright © 2022 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Authors do not have any conflicts. AG, CB, CP, MA, RK, MSE, MB are employees of OncoStem Diagnostics. Late GS has reported to have received honorarium from OncoStem Diagnostics. All other authors have no competing interests to declare.
Figures


References
-
- Turashvili G., Wen H.Y. Multigene testing in breast cancer: what have we learned from the 21-gene recurrence score assay? Breast J. 2020;26:1199–1207. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
