

A refined procedure for esophageal resection using a full minimally invasive approach
- PMID: 35246177
- PMCID: PMC8895824
- DOI: 10.1186/s13019-022-01765-2
A refined procedure for esophageal resection using a full minimally invasive approach
Abstract
Objective: Newer minimally invasive approaches to esophagectomy have brought substantial benefits to esophageal-cancer patients and continue to improve. We report here our experience with a streamlined procedure as part of a comprehensive perioperative-care program that provides additional advances in the continued evolution of this procedure.
Methods: All patients with primary esophageal cancer referred for resection to the Oakland Medical Center of the Kaiser-Permanente Northern California health plan who underwent this approach between January 2013 and August 2018 were included. Operative and clinical outcome variables were extracted from the electronic medical record, operating-room files, and manual chart review.
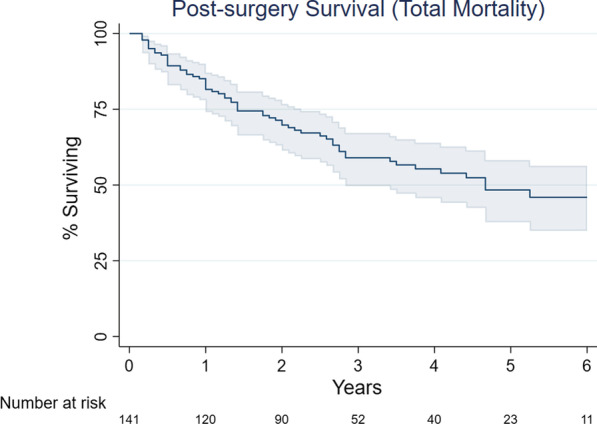
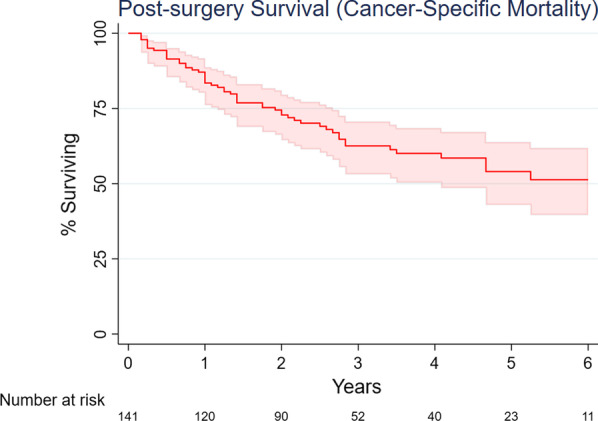
Results: 142 patients underwent the new procedure and care program; 121 (85.2%) were men with mean age of 64.5 years. 127 (89.4%) were adenocarcinoma; 117 (82.4%) were clinical stage III or IVA. 115 (81.0%) required no jejunostomy. Median hospital length-of-stay was 3 days and 8 (5.6%) patients required admission to the intensive care unit. Postoperative complications occurred in 22 (15.5%) patients within 30 days of the procedure. There were no inpatient deaths; one patient (0.7%) died within 30 days following discharge and three additional deaths (2.1%) occurred through 90 days of follow-up.
Conclusions: This approach resulted in excellent clinical outcomes, including short hospital stays with limited need for the intensive care unit, few perioperative complications, and relatively few patients requiring feeding tubes on discharge. This comprehensive approach to esophagectomy is feasible and provides another clinically meaningful advance in the progress of minimally invasive esophagectomy. Further development and dissemination of this method is warranted.
Keywords: Esophageal cancer; Esophagectomy; Minimally invasive surgery.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68(1):7–30. - PubMed
-
- Esophageal Cancer—Cancer Stat Facts. SEER [cited 2019 Apr 11]. https://seer.cancer.gov/statfacts/html/esoph.html.
-
- Ra J, Paulson EC, Kucharczuk J, Armstrong K, Wirtalla C, Rapaport-Kelz R, et al. Postoperative mortality after esophagectomy for cancer: development of a preoperative risk prediction model. Ann Surg Oncol. 2008;15(6):1577–1584. - PubMed
