

Gender differences in cardiometabolic health and disease in a cross-sectional observational obesity study
- PMID: 35246259
- PMCID: PMC8897897
- DOI: 10.1186/s13293-022-00416-4
Gender differences in cardiometabolic health and disease in a cross-sectional observational obesity study
Abstract
Background: Beyond the degree of adiposity, the pattern of fat distribution has a profound influence on cardiometabolic risk. It is unclear if sex differences in body fat distribution can potentially explain any sex differences in the prevalence of the metabolic syndrome (MetS) and in individual cardiometabolic risk factors among obese men and women.
Methods: In this cross-sectional analysis, 432 persons from the ongoing Obesity Weight Reduction Study (n = 356 obese, ØBMI 41 ± 8 kg/m2, and 76 non-obese, ØBMI 25 ± 3 kg/m2), were included. The relations of sex to MetS prevalence and selected cardiometabolic risk factors were assessed using univariate and multivariate adjusted regression models.
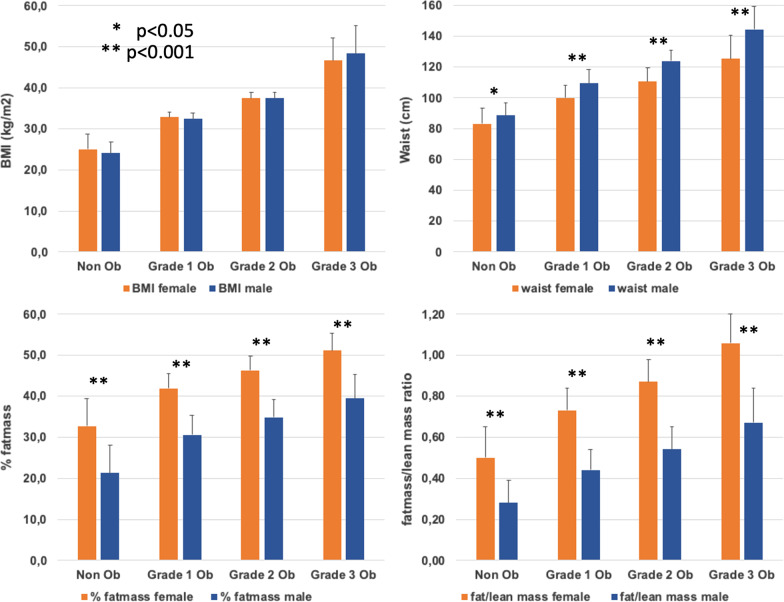
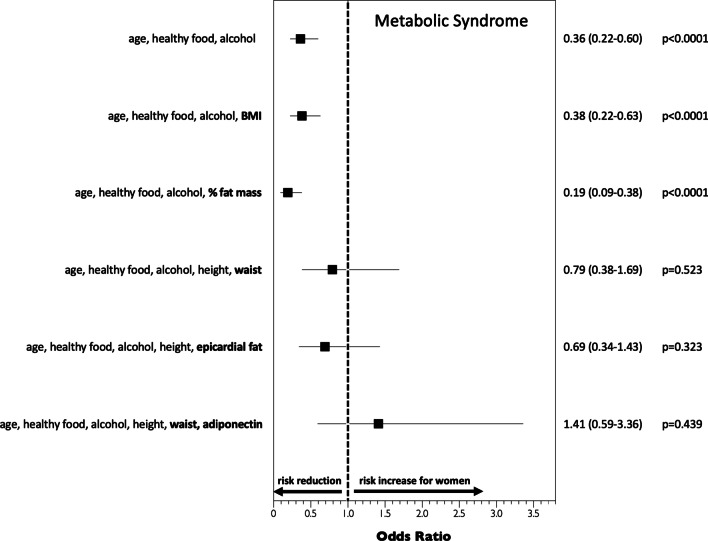
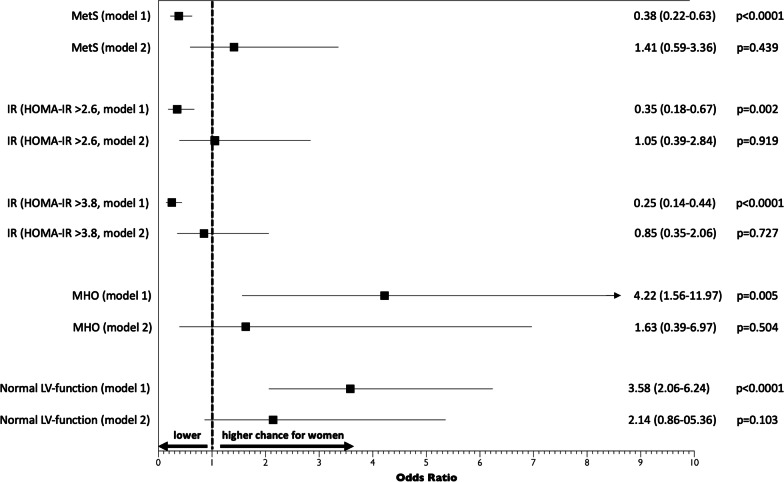
Results: In crude analyses, %fat mass and the fat mass/lean mass ratio were significantly higher in women than in men, regardless of increasing obesity categories, from normal weight to grade-3-obesity. In contrast, markers of abdominal obesity, such as waist circumference and waist-to-hip ratio were higher in men than in women, despite similar BMI. The prevalence of the MetS was higher in obese men than in women (67.6 vs. 45.0%, p < 0.0001), particularly in younger individuals < 40 years (72.5 vs. 36.8%, p < 0.0001), but "metabolically healthy obesity" (BMI ≥ 30, no other NCEP ATPIII MetS component) was more common in women than in men (15.6 vs. 4.1%, p < 0.0001). After adjusting for age, %body fat and height, sex differences were observed for HDL-cholesterol (p < 0.001), triglycerides (p < 0.001), fasting glucose (p = 0.002), insulin and HOMA-IR levels (p < 0.001), ALAT (p < 0.001), adiponectin (p < 0.001), and sE-selectin (p = 0.005). In contrast, crude sex differences in other variables, such as leptin levels (68 ± 4 in obese women vs. 33 ± 2 µg/L in men, p < 0.0001), disappeared after accounting for differences in %body fat (least-squares means of leptin: 52 ± 4 vs. 55 ± 6 µg /L, p = 0.740). A logistic regression model adjusting for age and lifestyle factors revealed a lower risk of having MetS for women as compared to men (OR = 0.38[0.22-0.60]). That risk estimate did not materially alter after adding BMI to the model. In contrast, no statistically significant association between sex and MetS prevalence was observed after adding waist circumference and adiponectin to the model (OR = 1.41[0.59-3.36]).
Conclusions: Different body fat distribution patterns, particularly abdominal adiposity, adiponectin, and related biomarkers, may contribute to sex differences in cardiometabolic risk factors and to the prevalence of the MetS.
Keywords: Adiponectin; Body fat distribution; Cardiometabolic health; Metabolic syndrome; Sex differences.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Eckel RH, Grundy SM, Zimmet PZ. The metabolic syndrome. Lancet. 2005;365(9468):1415–1428. - PubMed
-
- Stefan N, Kantartzis K, Machann J, Schick F, Thamer C, Rittig K, et al. Identification and characterization of metabolically benign obesity in humans. Arch Intern Med. 2008;168(15):1609–1616. - PubMed
-
- Romacho T, Elsen M, Rohrborn D, Eckel J. Adipose tissue and its role in organ crosstalk. Acta Physiol (Oxf) 2014;210(4):733–753. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
