

Evaluation of response to 13-valent conjugated pneumococcal vaccination in patients with rheumatoid arthritis receiving upadacitinib: results from a phase 2 open-label extension study
- PMID: 35246470
- PMCID: PMC8900062
- DOI: 10.1136/rmdopen-2021-002110
Evaluation of response to 13-valent conjugated pneumococcal vaccination in patients with rheumatoid arthritis receiving upadacitinib: results from a phase 2 open-label extension study
Abstract
Objective: To assess the immunogenicity of pneumococcal 13-valent conjugate vaccination (PCV-13) in patients with rheumatoid arthritis receiving upadacitinib and background methotrexate (MTX).
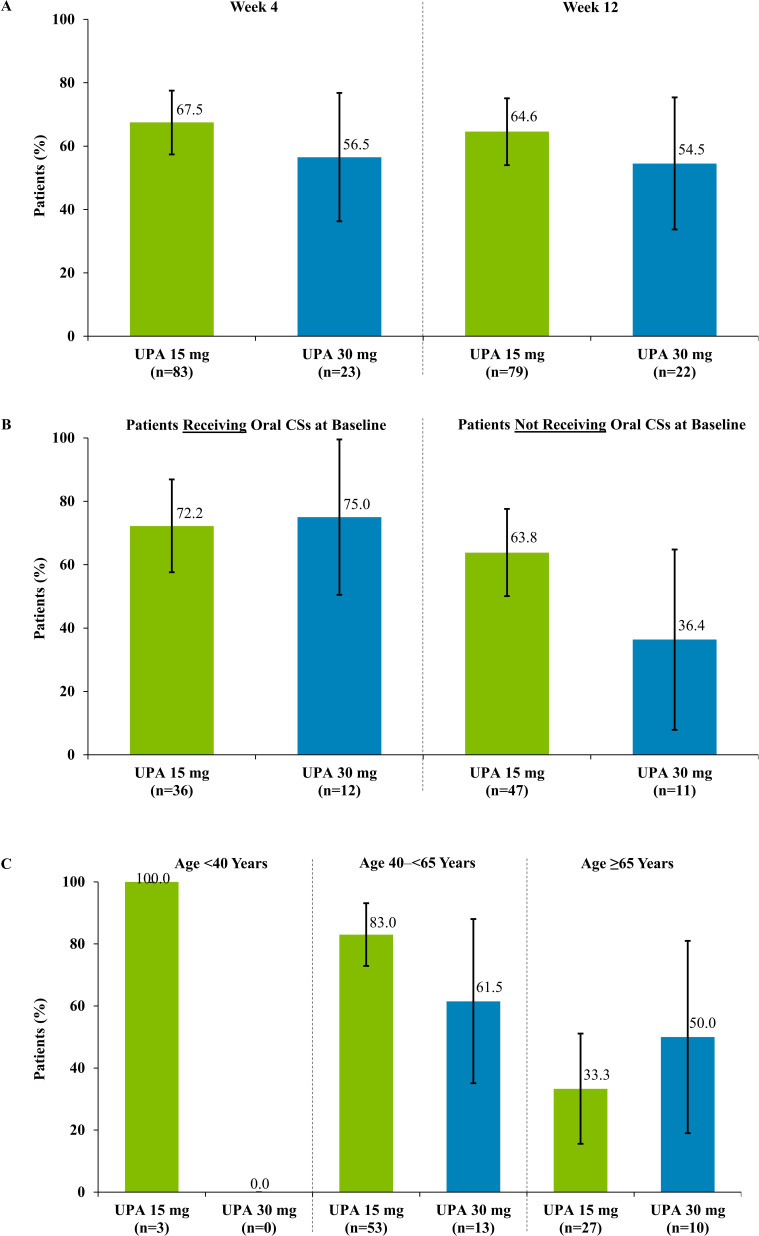
Methods: Eligible patients from the phase 2 open-label extension trial BALANCE-EXTEND (NCT02049138) receiving stable dosing of upadacitinib 15 mg or 30 mg once daily plus background MTX were given PCV-13. Antibody titres were collected prevaccination and 4 and 12 weeks postvaccination. The primary endpoint was the proportion of patients with satisfactory humoral response to PCV-13, defined as a ≥2-fold increase in ≥6 of 12 pneumococcal antigens at 4 weeks postvaccination.
Results: Of 111 patients (upadacitinib 15 mg, N=87; 30 mg, N=24), 85.6% were women, 97.3% used concomitant MTX and 44.1% used oral corticosteroids. At 4 weeks, 67.5% (95% CI 57.4 to 77.5) of patients receiving upadacitinib 15 mg and 56.5% (36.3 to 76.8) receiving 30 mg had a satisfactory PCV-13 response. Responses were similar in patients who used or did not use concomitant corticosteroids. No deaths or serious adverse events were reported.
Conclusions: Approximately two-thirds of patients receiving upadacitinib 15 mg once daily achieved a satisfactory humoral response to PCV-13 despite receiving concomitant MTX. Concomitant corticosteroid use did not negatively affect PCV-13 response.
Keywords: antirheumatic agents; arthritis; rheumatoid; vaccination.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: KW has received consulting fees and/or grant/research support from AbbVie, AstraZeneca, Bristol-Myers Squibb, Eli Lilly and Company, Galapagos, Gilead, GlaxoSmithKline, Novartis, Pfizer, Regeneron, Roche, Sanofi and UCB; and is an editorial board member of RMD Open.JI Vargas has received honoraria from AbbVie and fees from AbbVie as Principal Investigator in the study. ED has received fees from AbbVie as Principal Investigator in the study. CG has received fees from AbbVie as Principal Investigator in the study. AF, BH, YL and JK are employees of AbbVie and may own stocks or options. AK has received consulting fees and/or honoraria from AbbVie, Amgen, Boehringer Ingelheim, Eli Lilly and Company, Flexion, Genzyme, Gilead, Horizon, Janssen, Merck, Novartis, Pfizer, Regeneron, Sanofi, Sanofi Aventis, SUN Pharma Advanced Research, and UCB; owns stocks or options in Amgen, Gilead, GlaxoSmithKline, Novartis, Pfizer, and Sanofi; his institution received fees from AbbVie for his role as a Principal Investigator in the study.
Figures
References
-
- Singh JA, Saag KG, SL BJ. American College of rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Care Res 2015;2016:1–25. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical