

Eculizumab versus rituximab in generalised myasthenia gravis
- PMID: 35246490
- PMCID: PMC9016243
- DOI: 10.1136/jnnp-2021-328665
Eculizumab versus rituximab in generalised myasthenia gravis
Abstract
Objective: Myasthenia gravis (MG) is the most common autoimmune disorder affecting the neuromuscular junction. However, evidence shaping treatment decisions, particularly for treatment-refractory cases, is sparse. Both rituximab and eculizumab may be considered as therapeutic options for refractory MG after insufficient symptom control by standard immunosuppressive therapies.
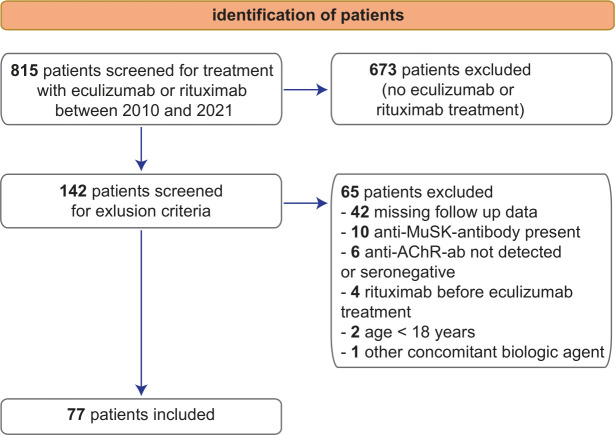
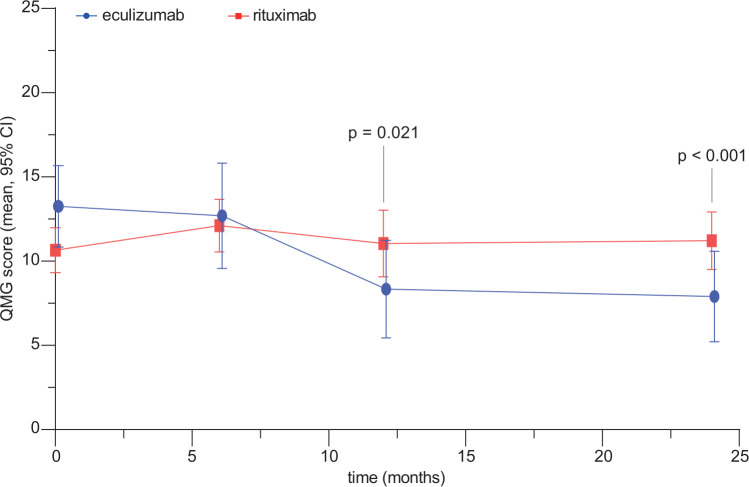
Methods: In this retrospective observational study, we included 57 rituximab-treated and 20 eculizumab-treated patients with MG to compare the efficacy of treatment agents in generalised, therapy-refractory anti-acetylcholine receptor antibody (anti-AChR-ab)-mediated MG with an observation period of 24 months. Change in the quantitative myasthenia gravis (QMG) score was defined as the primary outcome parameter. Differences between groups were determined in an optimal full propensity score matching model.
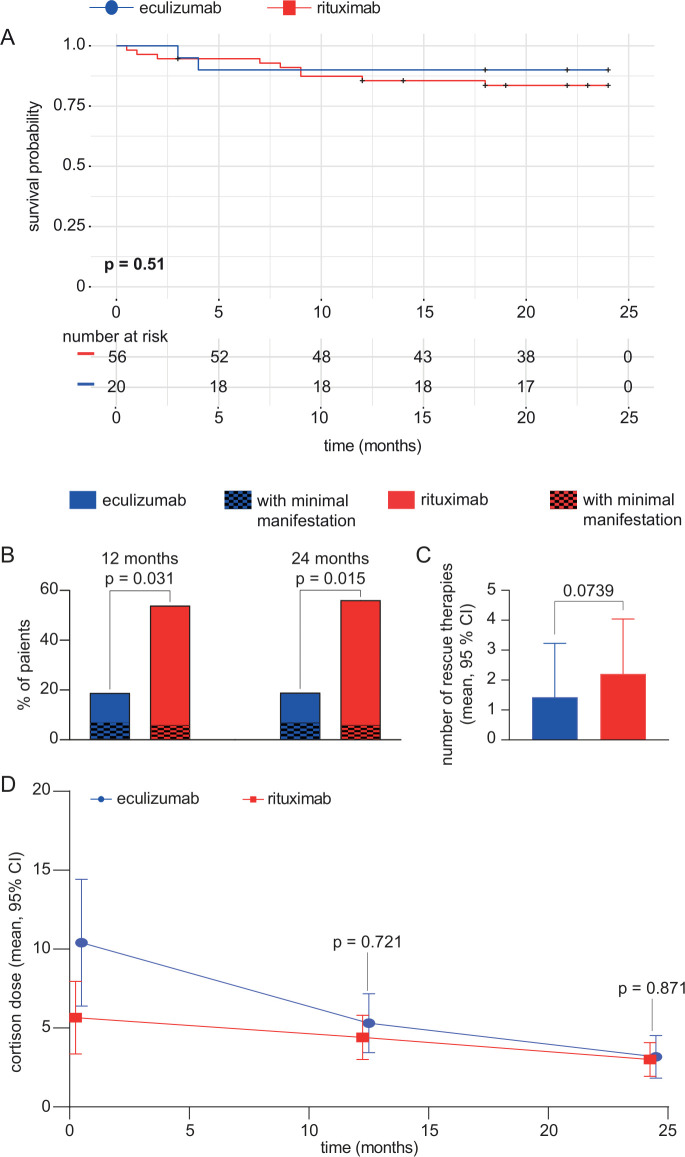
Results: Both groups were comparable in terms of clinical and demographic characteristics. Eculizumab was associated with a better outcome compared with rituximab, as measured by the change of the QMG score at 12 and 24 months of treatment. Minimal manifestation of disease was more frequently achieved in eculizumab-treated patients than rituximab-treated patients at 12 and 24 months after baseline. However, the risk of myasthenic crisis (MC) was not ameliorated in either group.
Interpretation: This retrospective, observational study provides the first real-world evidence supporting the use of eculizumab for the treatment of refractory, anti-AChR-ab positive MG. Nonetheless, the risk of MC remained high and prompts the need for intensified monitoring and further research effort aimed at this vulnerable patient cohort.
Keywords: myasthenia; neuroimmunology; neuromuscular.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: CN reports no conflicts of interest. CBS reports no conflicts of interest. FS received speaking honoraria from Biogen and Alexion. MP received speaker honoraria and travel/accommodation/meeting expenses from Novartis. LR-N reports no disclosures. NM reports no conflicts of interest. PM is on the Advisory Board of HealthNextGen and has equity interest in the company. His research is funded by the Bundesministerium für Bildung und Forschung (BMBF), the European Union, the Else Kröner-Fresenius Stiftung, the Volkswagen Stiftung and the Einstein Foundation Berlin. AG reports no conflicts of interest. HS reports no conflicts of interest. MS reports no conflicts of interest. BB received travel grants and/or training expenses from Bayer Vital GmbH, IpsenPharma GmbH, Norvartis, Biogen GmbH and Genzyme, as well as lecture fees from Ipsen Pharma GmbH, Alexion Pharma GmbH, Merck, Sanofi Genzyme and Roche. AT reports on conflicts of interest. TH received speaker honoraria and advisor honoraria from Alexion, Argenx, Biogen, Roche, Sanofi-Genzyme, Novartis and Hormosan. SS reports no conflicts of interest. SV reports no conflicts of interest. AM received speaker honoraria, consulting services and/or research support research from Alexion, argnx, GRIFOLS, Hormosan, Janssen, Octapharma, UCB and Vitaccess. He serves as chairman of the medical advisory board of the German Myasthenia Gravis Society. HW receives honoraria for acting as a member of Scientific Advisory Boards, Biogen, Evgen, Genzyme, MedDay Pharmaceuticals, Merck Serono, Novartis, Roche Pharma AG and Sanofi-Aventis as well as speaker honoraria and travel support from Alexion, Biogen, Cognomed, F. Hoffmann-La Roche, Gemeinnützige Hertie-Stiftung, Merck Serono, Novartis, Roche Pharma AG, Genzyme, TEVA and WebMD Global. HW is acting as a paid consultant for AbbVie, Actelion, Biogen, IGES, Johnson & Johnson, Novartis, Roche, Sanofi-Aventis and the Swiss Multiple Sclerosis Society. His research is funded by the German Ministry for Education and Research (BMBF), Deutsche Forschungsgemeinschaft (DFG), Else Kröner Fresenius Foundation, Fresenius Foundation, the European Union, Hertie Foundation, NRW Ministry of Education and Research, Interdisciplinary Center for Clinical Studies (IZKF) Muenster and RE Children’s Foundation, Biogen, GlaxoSmithKline GmbH, Roche Pharma AG, Sanofi-Genzyme. SGM receives honoraria for lecturing, and travel expenses for attending meetings from Almirall, Amicus Therapeutics Germany, Bayer Health Care, Biogen, Celgene, Diamed, Genzyme, MedDay Pharmaceuticals, Merck Serono, Novartis, Novo Nordisk, ONO Pharma, Roche, Sanofi-Aventis, Chugai Pharma, QuintilesIMS and Teva. His research is funded by the German Ministry for Education and Research (BMBF), Bundesinstitut für Risikobewertung (BfR), Deutsche Forschungsgemeinschaft (DFG), Deutsche Multiple Sklerose Gesellschaft (DMSG), Else Kröner Fresenius Foundation, Gemeinsamer Bundesausschuss (G-BA), German Academic Exchange Service, Hertie Foundation, Interdisciplinary Center for Clinical Studies (IZKF) Muenster, German Foundation Neurology and Alexion, Almirall, Amicus Therapeutics Germany, Biogen, Diamed, Fresenius Medical Care, Genzyme, HERZ Burgdorf, Merck Serono, Novartis, ONO Pharma, Roche and Teva. HW receives honoraria for acting as a member of Scientific Advisory Boards, Biogen, Evgen, Genzyme, MedDay Pharmaceuticals, Merck Serono, Novartis, Roche Pharma AG and Sanofi-Aventis as well as speaker honoraria and travel support from Alexion, Biogen, Cognomed, F. Hoffmann-La Roche, Gemeinnützige Hertie-Stiftung, Merck Serono, Novartis, Roche Pharma AG, Genzyme, TEVA and WebMD Global. TR reports grants from German Ministry of Education, Science, Research and Technology, grants and personal fees from Sanofi-Genzyme and Alexion; personal fees from Biogen, Roche and Teva; personal fees and non-financial support from Merck Serono, outside the submitted work.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical