

A reference set of clinically relevant adverse drug-drug interactions
- PMID: 35246559
- PMCID: PMC8897500
- DOI: 10.1038/s41597-022-01159-y
A reference set of clinically relevant adverse drug-drug interactions
Abstract
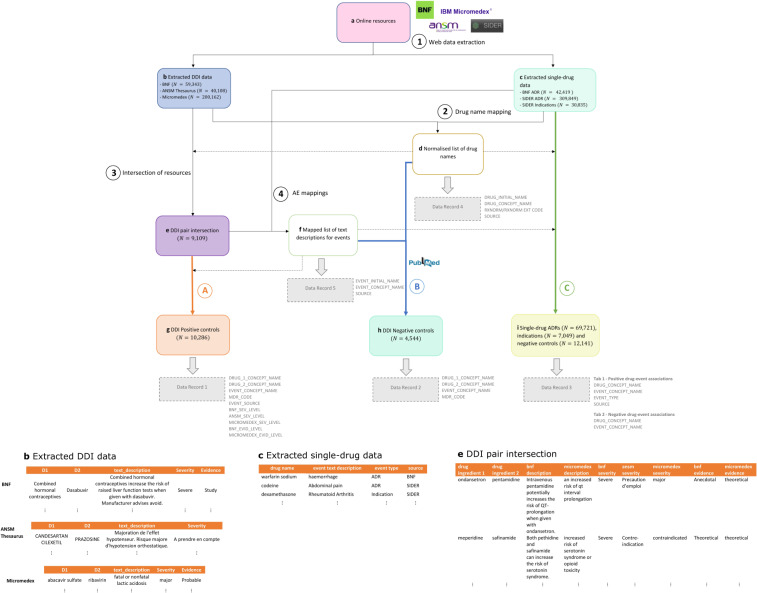
The accurate and timely detection of adverse drug-drug interactions (DDIs) during the postmarketing phase is an important yet complex task with potentially major clinical implications. The development of data mining methodologies that scan healthcare databases for drug safety signals requires appropriate reference sets for performance evaluation. Methodologies for establishing DDI reference sets are limited in the literature, while there is no publicly available resource simultaneously focusing on clinical relevance of DDIs and individual behaviour of interacting drugs. By automatically extracting and aggregating information from multiple clinical resources, we provide a scalable approach for generating a reference set for DDIs that could support research in postmarketing safety surveillance. CRESCENDDI contains 10,286 positive and 4,544 negative controls, covering 454 drugs and 179 adverse events mapped to RxNorm and MedDRA concepts, respectively. It also includes single drug information for the included drugs (i.e., adverse drug reactions, indications, and negative drug-event associations). We demonstrate usability of the resource by scanning a spontaneous reporting system database for signals of DDIs using traditional signal detection algorithms.
© 2022. The Author(s).
Conflict of interest statement
EK receives PhD studentship that is jointly funded by AstraZeneca and the EPSRC. MP receives research funding from various organizations including the MRC and NIHR. He has also received partnership funding for the MRC Clinical Pharmacology Training Scheme (co-funded by MRC and Roche, UCB, Eli Lilly and Novartis) and grant funding from Vistagen Therapeutics. He has also unrestricted educational grant support for the UK Pharmacogenetics and Stratified Medicine Network from Bristol-Myers Squibb and UCB. He has developed an HLA genotyping panel with MC Diagnostics, but does not benefit financially from this. He is part of the IMI Consortium ARDAT (
Figures
References
-
- National Center for Health Statistics. Health, United States, 2019. (2021). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
