

From a Symptom-Based to a Mechanism-Based Pharmacotherapeutic Treatment in Complex Regional Pain Syndrome
- PMID: 35247200
- PMCID: PMC9016036
- DOI: 10.1007/s40265-022-01685-4
From a Symptom-Based to a Mechanism-Based Pharmacotherapeutic Treatment in Complex Regional Pain Syndrome
Abstract
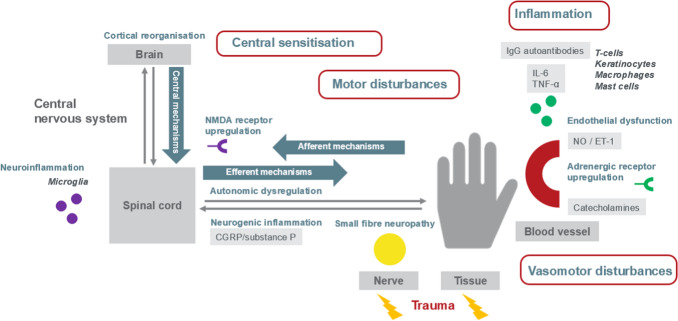
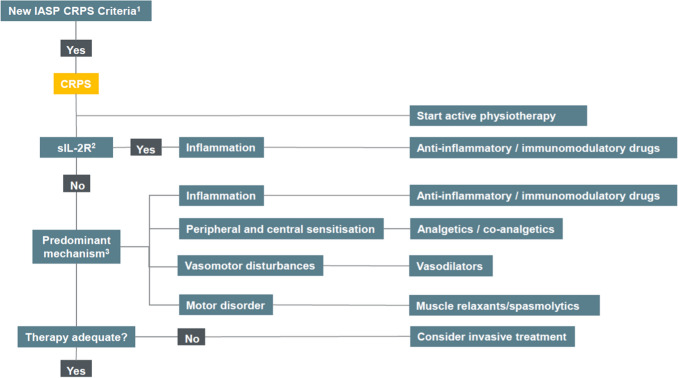
Complex regional pain syndrome (CRPS) is a debilitating painful condition of a distal extremity that can develop after tissue damage. CRPS is thought to be a multimechanism syndrome and ideally the most prominent mechanism(s) should be targeted by drugs in an individually tailored manner. This review gives an overview of the action and evidence of current and future pharmacotherapeutic options for CRPS. The available options are grouped in four categories by their therapeutic actions on the CRPS mechanisms, i.e. inflammation, central sensitisation, vasomotor disturbances and motor disturbances. More knowledge about the underlying mechanisms of CRPS helps to specifically target important CRPS mechanisms. In the future, objective biomarkers could potentially aid in selecting appropriate mechanism-based drugs in order to increase the effectiveness of CRPS treatment. Using this approach, current and future pharmacotherapeutic options for CRPS should be studied in multicentre trials to prove their efficacy. The ultimate goal is to shift the symptom-based selection of therapy into a mechanism-based selection of therapy in CRPS.
© 2022. The Author(s).
Conflict of interest statement
Frank J.P.M. Huygen reports personal fees from Abbott; grants and personal fees from Saluda; and personal fees from Boston Scientific, Grunenthal, and Pfizer outside the submitted work. Thomas J.P. Mangnus, Krishna D. Bharwani, and Maaike Dirckx report no other conflicts of interest that are relevant to the contents of this article.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
