

BMI and Treatment Response in Patients With Pulmonary Arterial Hypertension: A Meta-analysis
- PMID: 35247393
- PMCID: PMC9470735
- DOI: 10.1016/j.chest.2022.02.041
BMI and Treatment Response in Patients With Pulmonary Arterial Hypertension: A Meta-analysis
Abstract
Background: Obesity is increasingly prevalent in pulmonary arterial hypertension (PAH) but is associated with improved survival, creating an "obesity paradox" in PAH. It is unknown if the improved outcomes could be attributable to obese patients deriving a greater benefit from PAH therapies.
Research question: Does BMI modify treatment effectiveness in PAH?
Study design and methods: Using individual participant data, a meta-analysis was conducted of phase III, randomized, placebo-controlled trials of treatments for PAH submitted for approval to the U.S. Food and Drug Administration from 2000 to 2015. Primary outcomes were change in 6-min walk distance (6MWD) and World Health Organization (WHO) functional class.
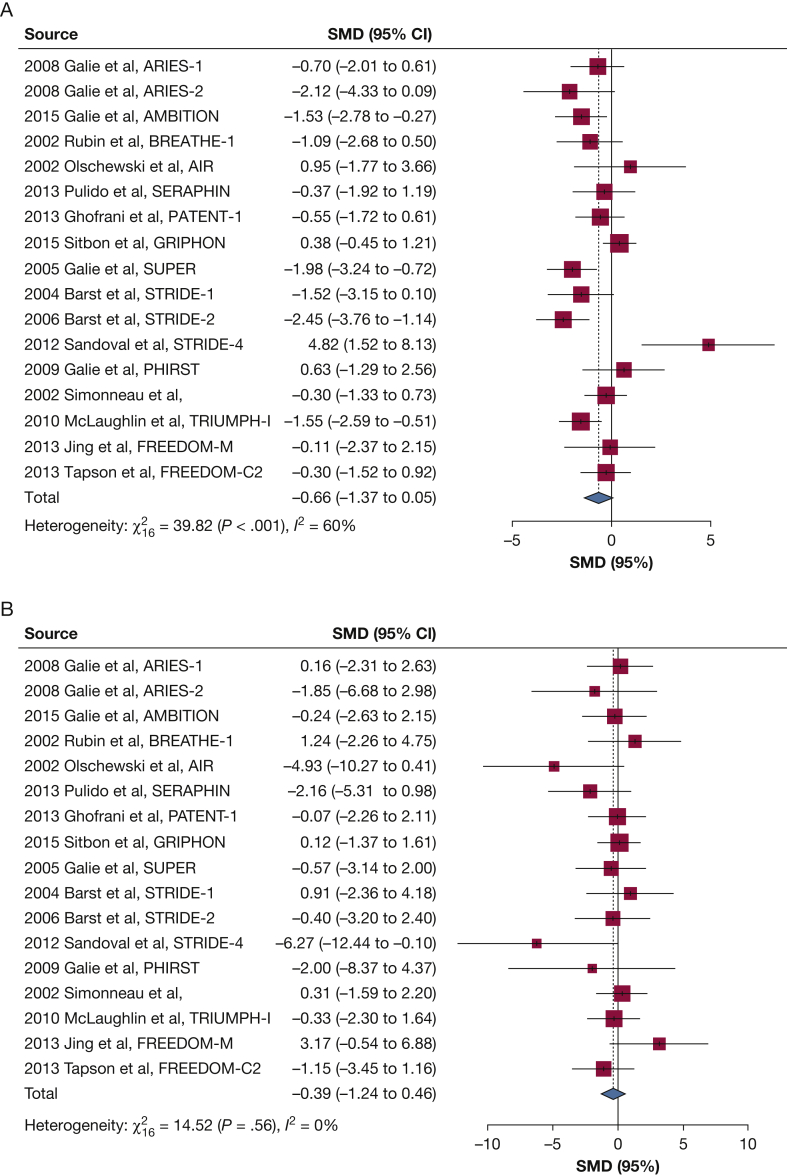
Results: A total of 5,440 participants from 17 trials were included. Patients with overweight and obesity had lower baseline 6MWD and were more likely to be WHO functional class III or IV. Treatment was associated with a 27.01-m increase in 6MWD (95% CI, 21.58-32.45; P < .001) and lower odds of worse WHO functional class (OR, 0.58; 95% CI, 0.48-0.70; P < .001). For every 1 kg/m2 increase in BMI, 6MWD was reduced by 0.66 m (P = .07); there was no significant effect modification of treatment response in 6MWD according to BMI (P for interaction = .34). Higher BMI was not associated with odds of WHO functional class at end of follow-up; however, higher BMI attenuated the treatment response such that every 1 kg/m2 increase in BMI increased odds of worse WHO functional class by 3% (OR, 1.03; P for interaction = .06).
Interpretation: Patients with overweight and obesity had lower baseline 6MWD and worse WHO functional class than patients with normal weight with PAH. Higher BMI did not modify the treatment response for change in 6MWD, but it attenuated the treatment response for WHO functional class. PAH trials should include participants representative of all weight groups to allow for assessment of treatment heterogeneity and mechanisms.
Keywords: BMI; meta-analysis; obesity; pulmonary arterial hypertension.
Copyright © 2022 The Author(s). Published by Elsevier Inc. All rights reserved.
Figures



References
-
- Badesch D.B., Raskob G.E., Elliott C.G., et al. Pulmonary arterial hypertension: baseline characteristics from the REVEAL registry. Chest. 2010;137:376–387. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
