

Age is the main determinant of COVID-19 related in-hospital mortality with minimal impact of pre-existing comorbidities, a retrospective cohort study
- PMID: 35247983
- PMCID: PMC8897728
- DOI: 10.1186/s12877-021-02673-1
Age is the main determinant of COVID-19 related in-hospital mortality with minimal impact of pre-existing comorbidities, a retrospective cohort study
Abstract
Background: Age and comorbidities increase COVID-19 related in-hospital mortality risk, but the extent by which comorbidities mediate the impact of age remains unknown.
Methods: In this multicenter retrospective cohort study with data from 45 Dutch hospitals, 4806 proven COVID-19 patients hospitalized in Dutch hospitals (between February and July 2020) from the CAPACITY-COVID registry were included (age 69[58-77]years, 64% men). The primary outcome was defined as a combination of in-hospital mortality or discharge with palliative care. Logistic regression analysis was performed to analyze the associations between sex, age, and comorbidities with the primary outcome. The effect of comorbidities on the relation of age with the primary outcome was evaluated using mediation analysis.
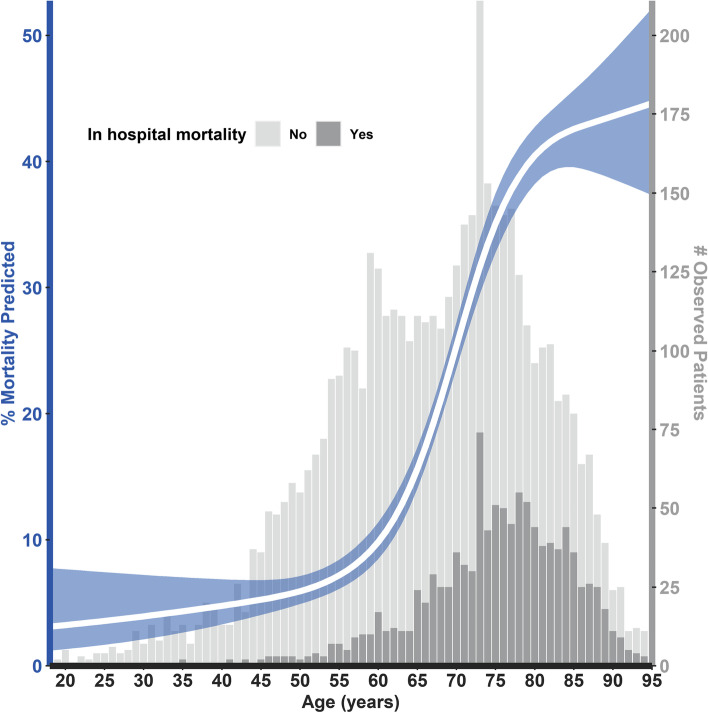
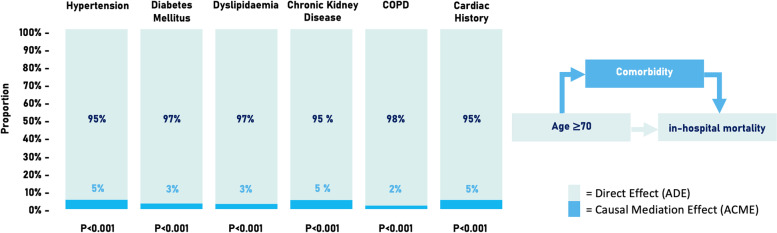
Results: In-hospital COVID-19 related mortality occurred in 1108 (23%) patients, 836 (76%) were aged ≥70 years (70+). Both age 70+ and female sex were univariably associated with outcome (odds ratio [OR]4.68, 95%confidence interval [4.02-5.45], OR0.68[0.59-0.79], respectively;both p< 0.001). All comorbidities were univariably associated with outcome (p<0.001), and all but dyslipidemia remained significant after adjustment for age70+ and sex. The impact of comorbidities was attenuated after age-spline adjustment, only leaving female sex, diabetes mellitus (DM), chronic kidney disease (CKD), and chronic pulmonary obstructive disease (COPD) significantly associated (female OR0.65[0.55-0.75], DM OR1.47[1.26-1.72], CKD OR1.61[1.32-1.97], COPD OR1.30[1.07-1.59]). Pre-existing comorbidities in older patients negligibly (<6% in all comorbidities) mediated the association between higher age and outcome.
Conclusions: Age is the main determinant of COVID-19 related in-hospital mortality, with negligible mediation effect of pre-existing comorbidities.
Trial registration: CAPACITY-COVID ( NCT04325412 ).
Keywords: COVID-19; Hospitalization; Mediation analysis; Mortality; Netherlands.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- WHO COVID-19 Dashboard. Geneva: World Health Organization, 2020. Available online: https://covid19.who.int/ (last cited: 16-07-2021).
-
- NHS Digital . Coronavirus (COVID-19): shielded patients list. 2020.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
