

Prognostic effects of treatment protocols for febrile convulsive status epilepticus in children
- PMID: 35247987
- PMCID: PMC8897930
- DOI: 10.1186/s12883-022-02608-2
Prognostic effects of treatment protocols for febrile convulsive status epilepticus in children
Abstract
Background: Febrile status epilepticus is the most common form of status epilepticus in children. No previous reports compare the effectiveness of treatment strategies using fosphenytoin (fPHT) or phenobarbital (PB) and those using anesthetics as second-line anti-seizure medication for benzodiazepine-resistant convulsive status epilepticus (CSE). We aimed to examine the outcomes of various treatment strategies for febrile convulsive status epilepticus (FCSE) in a real-world setting while comparing the effects of different treatment protocols and their presence or absence.
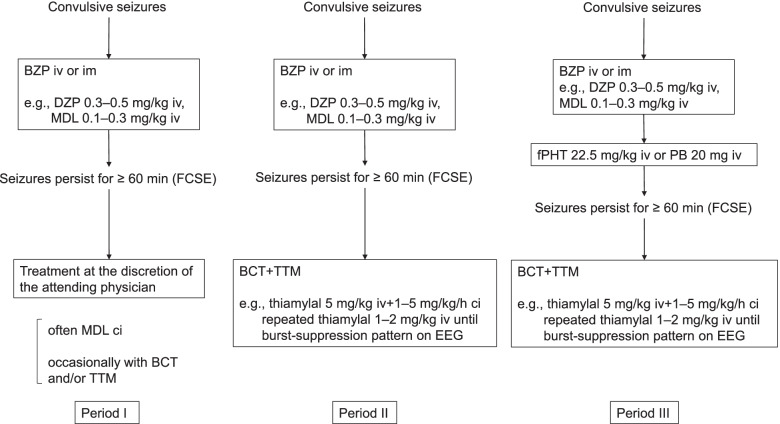
Methods: This was a single-center historical cohort study that was divided into three periods. Patients who presented with febrile convulsive status epilepticus for ≥60 min even after the administration of at least one anticonvulsant were included. During period I (October 2002-December 2006), treatment was performed at the discretion of the attending physician, without a protocol. During period II (January 2007-February 2013), barbiturate coma therapy (BCT) was indicated for FCSE resistant to benzodiazepines. During period III (March 2013-April 2016), BCT was indicated for FCSE resistant to fPHT or PB.
Results: The rate of electroencephalogram monitoring was lower in period I than period II+III (11.5% vs. 85.7%, p<0.01). Midazolam was administered by continuous infusion more often in period I than period II+III (84.6% vs. 25.0%, p<0.01), whereas fPHT was administered less often in period I than period II+III (0% vs. 27.4%, p<0.01). The rate of poor outcome, which was determined using the Pediatric Cerebral Performance Category scale, was higher in period I than period II+III (23.1% vs. 7.1%, p=0.03). The rate of poor outcome did not differ between periods II and III (4.2% vs. 11.1%, p=0.40).
Conclusions: While the presence of a treatment protocol for FCSE in children may improve outcomes, a treatment protocol using fPHT or PB may not be associated with better outcomes.
Keywords: Anticonvulsant; Barbiturate; Benzodiazepine; Clinical protocol; Febrile seizure; Phenytoin.
© 2022. The Author(s).
Conflict of interest statement
The authors have no financial relationships relevant to this article to disclose. Potential conflicts of interest: Kazumoto Iijima has received grants from Eisai Co., Ltd, and consulting fees from Takeda P Pharma Co., Ltd.; Kandai Nozu has received consulting fees from Eisai Co., Ltd, and lecture fees from Sumitomo Dainippon Pharma Co., Ltd. There is no potential conflict of interest by the rest of the authors.
Figures

Similar articles
-
Fosphenytoin vs. continuous midazolam for pediatric febrile status epilepticus.Brain Dev. 2018 Nov;40(10):884-890. doi: 10.1016/j.braindev.2018.08.001. Epub 2018 Aug 23. Brain Dev. 2018. PMID: 30144969
-
Efficacy of levetiracetam versus fosphenytoin for the recurrence of seizures after status epilepticus.Medicine (Baltimore). 2017 Jun;96(25):e7206. doi: 10.1097/MD.0000000000007206. Medicine (Baltimore). 2017. PMID: 28640109 Free PMC article.
-
A multicentre randomised controlled trial of levetiracetam versus phenytoin for convulsive status epilepticus in children (protocol): Convulsive Status Epilepticus Paediatric Trial (ConSEPT) - a PREDICT study.BMC Pediatr. 2017 Jun 22;17(1):152. doi: 10.1186/s12887-017-0887-8. BMC Pediatr. 2017. PMID: 28641582 Free PMC article. Clinical Trial.
-
[Management of convulsive status epilepticus in infants and children].Rev Neurol (Paris). 2009 Apr;165(4):390-7. doi: 10.1016/j.neurol.2008.11.009. Epub 2009 Mar 4. Rev Neurol (Paris). 2009. PMID: 19264335 Review. French.
-
Treatment of convulsive status epilepticus in infants and young children in Japan.Acta Neurol Scand Suppl. 2007;186:62-70. Acta Neurol Scand Suppl. 2007. PMID: 17784539 Review.
Cited by
-
Timing of therapeutic interventions against infection-triggered encephalopathy syndrome: a scoping review of the pediatric literature.Front Neurosci. 2023 Aug 22;17:1150868. doi: 10.3389/fnins.2023.1150868. eCollection 2023. Front Neurosci. 2023. PMID: 37674514 Free PMC article.
-
Epileptic Status in a PEDiatric cohort (ESPED) requiring intensive care treatment: A multicenter, national, two-year prospective surveillance study.Epilepsia Open. 2023 Jun;8(2):411-424. doi: 10.1002/epi4.12707. Epub 2023 Feb 20. Epilepsia Open. 2023. PMID: 36764666 Free PMC article.
References
-
- Glauser T, Shinnar S, Gloss D, Alldredge B, Arya R, Bainbridge J, et al. Evidence-based Guideline: Treatment of convulsive status epilepticus in children and adults: Report of the Guideline Committee of the American Epilepsy Society. Epilepsy Curr. 2016;16:48–61. doi: 10.5698/1535-7597-16.1.48. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
