

Anti-tumor treatment and healthcare consumption near death in the era of novel treatment options for patients with melanoma brain metastases
- PMID: 35247992
- PMCID: PMC8897874
- DOI: 10.1186/s12885-022-09316-7
Anti-tumor treatment and healthcare consumption near death in the era of novel treatment options for patients with melanoma brain metastases
Abstract
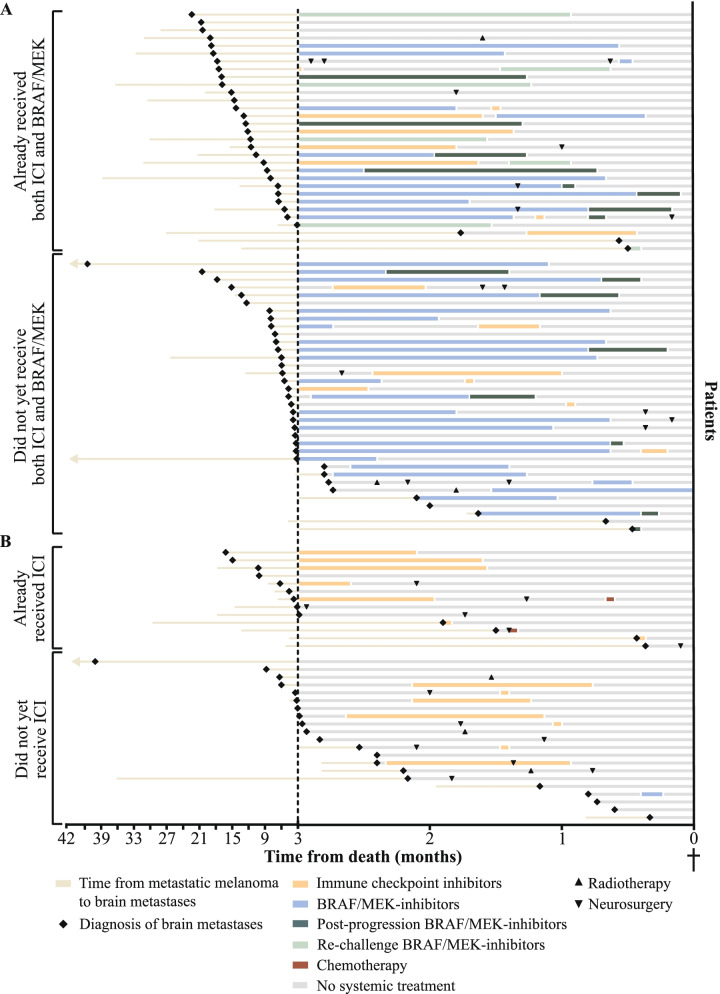
Background: Effective systemic treatments have revolutionized the management of patients with metastatic melanoma, including those with brain metastases. The extent to which these treatments influence disease trajectories close to death is unknown. Therefore, this study aimed to gain insight into provided treatments and healthcare consumption during the last 3 months of life in patients with melanoma brain metastases.
Methods: Retrospective, single-center study, including consecutive patients with melanoma brain metastases diagnosed between June-2015 and June-2018, referred to the medical oncologist, and died before November-2019. Patient and tumor characteristics, anti-tumor treatments, healthcare consumption, presence of neurological symptoms, and do-not-resuscitate status were extracted from medical charts.
Results: 100 patients were included. A BRAF-mutation was present in 66 patients. Systemic anti-tumor therapy was given to 72% of patients during the last 3 months of life, 34% in the last month, and 6% in the last week. Patients with a BRAF-mutation more frequently received systemic treatment during the last 3 (85% vs. 47%) and last month (42% vs. 18%) of life than patients without a BRAF-mutation. Furthermore, patients receiving systemic treatment were more likely to visit the emergency room (ER, 75% vs. 36%) and be hospitalized (75% vs. 36%) than those who did not.
Conclusion: The majority of patients with melanoma brain metastases received anti-tumor treatment during the last 3 months of life. ER visits and hospitalizations occurred more often in patients on anti-tumor treatment. Further research is warranted to examine the impact of anti-tumor treatments close to death on symptom burden and care satisfaction.
Keywords: Anti-tumor treatment; End-of-life care; Healthcare consumption; Melanoma; Neuro-oncology.
© 2022. The Author(s).
Conflict of interest statement
GAPH is a consultant/advisory board member for Amgen, Roche, Merck, Bristol-Myers Squibb, Pfizer, Novartis, and Pierre Fabre, and has received grants from Bristol-Myers Squibb and Seerave, outside the submitted work and paid to the institution. MJ has served as an advisory board member for Bristol-Myers Squibb, Novartis, Merck, and Pierre Fabre, fees paid to the institution. The other authors declare that they have no competing interests.
Figures
Similar articles
-
A Retrospective Evaluation of Vemurafenib as Treatment for BRAF-Mutant Melanoma Brain Metastases.Oncologist. 2015 Jul;20(7):789-97. doi: 10.1634/theoncologist.2014-0012. Epub 2015 May 8. Oncologist. 2015. PMID: 25956405 Free PMC article. Clinical Trial.
-
BRAF V600E mutation and BRAF kinase inhibitors in conjunction with stereotactic radiosurgery for intracranial melanoma metastases.J Neurosurg. 2017 Mar;126(3):726-734. doi: 10.3171/2016.2.JNS1633. Epub 2016 May 20. J Neurosurg. 2017. PMID: 27203149
-
Treatment patterns and outcomes in BRAF V600E-mutant melanoma patients with brain metastases receiving vemurafenib in the real-world setting.Cancer Med. 2015 Aug;4(8):1205-13. doi: 10.1002/cam4.475. Epub 2015 May 20. Cancer Med. 2015. PMID: 25991583 Free PMC article.
-
Multidisciplinary approach to brain metastasis from melanoma: the emerging role of systemic therapies.Am Soc Clin Oncol Educ Book. 2013:393-8. doi: 10.14694/EdBook_AM.2013.33.393. Am Soc Clin Oncol Educ Book. 2013. PMID: 23714558 Review.
-
Developments in the Space of New MAPK Pathway Inhibitors for BRAF-Mutant Melanoma.Clin Cancer Res. 2019 Oct 1;25(19):5735-5742. doi: 10.1158/1078-0432.CCR-18-0836. Epub 2019 Apr 16. Clin Cancer Res. 2019. PMID: 30992297 Free PMC article. Review.
Cited by
-
Systemic therapy timing and use in patients with advanced melanoma at the end of life: A retrospective cohort study.J Dermatol. 2024 Apr;51(4):584-591. doi: 10.1111/1346-8138.17061. Epub 2023 Dec 11. J Dermatol. 2024. PMID: 38078557 Free PMC article.
-
Real-World Evaluation of the Management, Treatment Pathways and Outcome of Melanoma Patients with Target Therapies in Italy.Adv Ther. 2023 Sep;40(9):3875-3895. doi: 10.1007/s12325-023-02578-y. Epub 2023 Jun 27. Adv Ther. 2023. PMID: 37368101 Free PMC article.
-
Systemic melanoma therapy at the end of life: A single institutional retrospective study in Japan.JAAD Int. 2022 Nov 11;10:51-52. doi: 10.1016/j.jdin.2022.11.001. eCollection 2023 Mar. JAAD Int. 2022. PMID: 36636101 Free PMC article. No abstract available.
References
-
- Gummadi T, Zhang BY, Valpione S, et al. Impact of BRAF mutation and BRAF inhibition on melanoma brain metastases. Melanoma Res. 2015;25:75–79. - PubMed
-
- Noone AM, Howlader N, Krapcho M, et al. Surveillance, Epidemiology, and End Results (SEER) Cancer Statistics Review, 1975-2015. Bethesda, MD; National Cancer Institute; 2018. Retrieved from www.seer.cancer.gov.
-
- Noh T, Walbert T. Brain metastasis: clinical manifestations, symptom management, and palliative care. Handb Clin Neurol. 2018;149:75–88. - PubMed
-
- Den RB, Andrews DW. Radiotherapy for brain metastases. Neurosurg Clin N Am. 2011;22:37–44. - PubMed
-
- Nieder C, Marienhagen K, Geinitz H, Grosu AL. Can current prognostic scores reliably guide treatment decisions in patients with brain metastases from malignant melanoma? J Cancer Res Ther. 2011;7:47–51. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
