

Cost-utility analysis of four WHO-recommended sofosbuvir-based regimens for the treatment of chronic hepatitis C in sub-Saharan Africa
- PMID: 35248039
- PMCID: PMC8897946
- DOI: 10.1186/s12913-021-07289-0
Cost-utility analysis of four WHO-recommended sofosbuvir-based regimens for the treatment of chronic hepatitis C in sub-Saharan Africa
Abstract
Background: Although direct-acting antivirals (DAA) have become standard care for patients with chronic hepatitis C worldwide, there is no evidence for their value for money in sub-Saharan Africa. We assessed the cost-effectiveness of four sofosbuvir-based regimens recommended by the World Health Organization (WHO) in Cameroon, Côte d'Ivoire and Senegal.
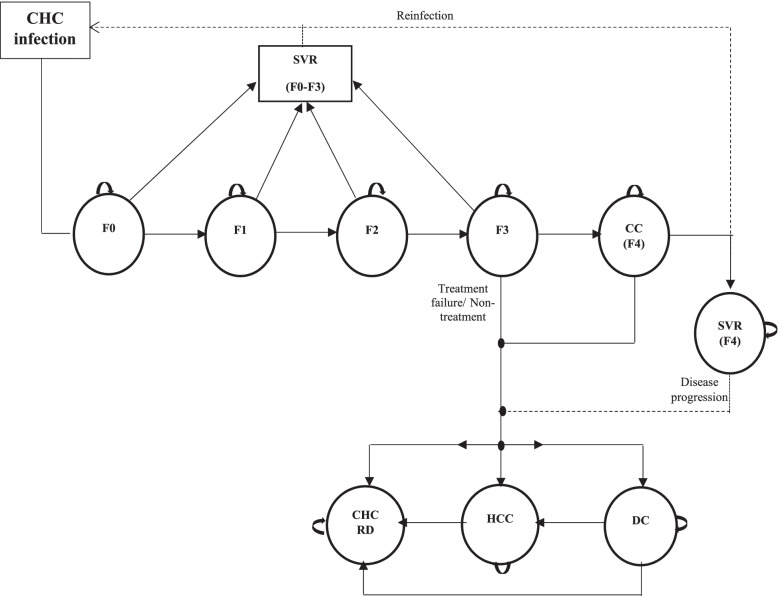
Methods: Using modelling, we simulated chronic hepatitis C progression with and without treatment in hypothetical cohorts of patients infected with the country's predominant genotypes (1, 2 and 4) and without other viral coinfections, history of liver complication or hepatocellular carcinoma. Using the status-quo 'no DAA treatment' as a comparator, we assessed four regimens: sofosbuvir-ribavirin, sofosbuvir-ledipasvir (both recommended in WHO 2016 guidelines and assessed in the TAC pilot trial conducted in Cameroon, Côte d'Ivoire and Senegal), sofosbuvir-daclatasvir and sofosbuvir-ledipasvir (two pangenotypic regimens recommended in WHO 2018 guidelines). DAA effectiveness, costs and utilities were mainly estimated using data from the TAC pilot trial. Secondary data from the literature was used to estimate disease progression probabilities with and without treatment. We considered two DAA pricing scenarios: S1) originator prices; S2) generic prices. Uncertainty was addressed using probabilistic and deterministic sensitivity analyses and cost-effectiveness acceptability curves.
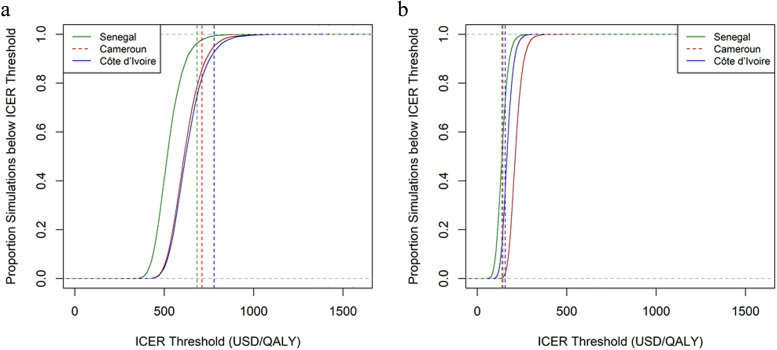
Results: With slightly higher effectiveness and significantly lower costs, sofosbuvir/velpatasvir was the preferred DAA regimen in S1 with incremental cost-effectiveness ratios (ICERs) ranging from US$526 to US$632/QALY. At the cost-effectiveness threshold (CET) of 0.5 times the 2017 country's per-capita gross domestic product (GDP), sofosbuvir/velpatasvir was only cost-effective in Senegal (probability > 95%). In S2 at generic prices, sofosbuvir/daclatasvir was the preferred regimen due to significantly lower costs. ICERs ranged from US$139 to US$216/QALY according to country i.e. a 95% probability of being cost-effective. Furthermore, this regimen was cost-effective (probability> 95%) for all CET higher than US$281/QALY, US$223/QALY and US$195/QALY in Cameroon, Côte d'Ivoire and Senegal, respectively, corresponding to 0.14 (Côte d'Ivoire and Senegal) and 0.2 (Cameroon) times the country's per-capita GDP.
Conclusions: Generic sofosbuvir/daclatasvir is very cost-effective for treating chronic hepatitis C in sub-Saharan Africa. Large-scale use of generics and an increase in national and international funding for hepatitis C treatment must be priorities for the HCV elimination agenda.
Keywords: Cameroon; Chronic hepatitis C; Cost-effectiveness analysis; Cost-utility analysis; Côte d’Ivoire; Direct-acting antivirals; Senegal; Sofosbuvir.
© 2022. The Author(s).
Conflict of interest statement
K.L. reports personal fees for advisory boards and travel grants from GILEAD and ABBVIE, all outside of the submitted work. All other authors report no conflict of interest in relation to this study.
Figures
References
-
- WHO . Global Hepatis report. 2017.
-
- Global Health estimates 2016: disease burden by cause, age, sex, by country and by region, 2000-2016. World Health Organization; 2018. https://www.who.int/healthinfo/global_burden_disease/estimates/en/index1.... Accessed 20 Sept 2018.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
