

MRI-based contrast clearance analysis shows high differentiation accuracy between radiation-induced reactions and progressive disease after cranial radiotherapy
- PMID: 35248822
- PMCID: PMC9058918
- DOI: 10.1016/j.esmoop.2022.100424
MRI-based contrast clearance analysis shows high differentiation accuracy between radiation-induced reactions and progressive disease after cranial radiotherapy
Abstract
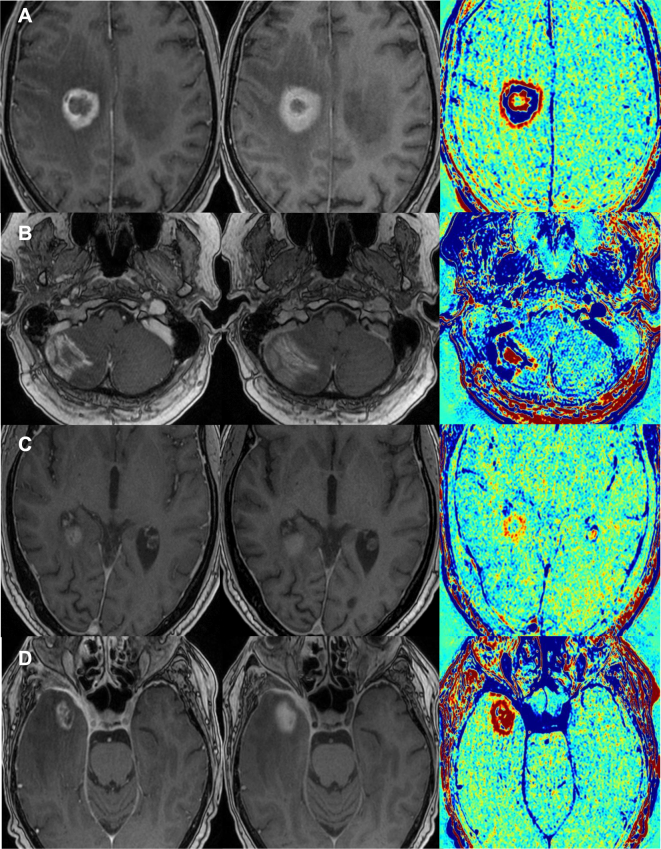
Background: Pseudoprogression (PsP) or radiation necrosis (RN) may frequently occur after cranial radiotherapy and show a similar imaging pattern compared with progressive disease (PD). We aimed to evaluate the diagnostic accuracy of magnetic resonance imaging-based contrast clearance analysis (CCA) in this clinical setting.
Patients and methods: Patients with equivocal imaging findings after cranial radiotherapy were consecutively included into this monocentric prospective study. CCA was carried out by software-based automated subtraction of imaging features in late versus early T1-weighted sequences after contrast agent application. Two experienced neuroradiologists evaluated CCA with respect to PsP/RN and PD being blinded for histological findings. The radiological assessment was compared with the histopathological results, and its accuracy was calculated statistically.
Results: A total of 33 patients were included; 16 (48.5%) were treated because of a primary brain tumor (BT), and 17 (51.1%) because of a secondary BT. In one patient, CCA was technically infeasible. The accuracy of CCA in predicting the histological result was 0.84 [95% confidence interval (CI) 0.67-0.95; one-sided P = 0.051; n = 32]. Sensitivity and specificity of CCA were 0.93 (95% CI 0.66-1.00) and 0.78 (95% CI 0.52-0.94), respectively. The accuracy in patients with secondary BTs was 0.94 (95% CI 0.71-1.00) and nonsignificantly higher compared with patients with primary BT with an accuracy of 0.73 (95% CI 0.45-0.92), P = 0.16.
Conclusions: In this study, CCA was a highly accurate, easy, and helpful method for distinguishing PsP or RN from PD after cranial radiotherapy, especially in patients with secondary tumors after radiosurgical treatment.
Keywords: brain metastases; glioma; pseudoprogression; radiation necrosis; stereotactic radiosurgery.
Copyright © 2022 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Disclosure RB, IH, DFF, JM, SC, CB,MN: Brainlab (Munich, Germany) holds a framework contract with the Department of Radiation Oncology, University Hospital LMU Munich, and specific research projects are financially supported not directly related to the current project. All other authors have declared no conflicts of interest.
Figures
Similar articles
-
Histopathological correlation of brain tumor recurrence vs. radiation effect post-radiosurgery as detected by MRI contrast clearance analysis: a validation study.J Neurooncol. 2024 Jul;168(3):547-553. doi: 10.1007/s11060-024-04697-0. Epub 2024 May 15. J Neurooncol. 2024. PMID: 38748050
-
MR perfusion characteristics of pseudoprogression in brain tumors treated with immunotherapy - a comparative study with chemo-radiation induced pseudoprogression and radiation necrosis.J Neurooncol. 2025 Mar;172(1):239-247. doi: 10.1007/s11060-024-04910-0. Epub 2024 Dec 17. J Neurooncol. 2025. PMID: 39688766 Free PMC article.
-
Investigating the role of delayed contrast magnetic resonance imaging (MRI) to differentiate radiation necrosis from tumour recurrence in brain metastases after stereotactic radiosurgery.J Med Imaging Radiat Oncol. 2023 Apr;67(3):292-298. doi: 10.1111/1754-9485.13504. Epub 2023 Jan 17. J Med Imaging Radiat Oncol. 2023. PMID: 36650724
-
Bevacizumab for radiation necrosis following radiotherapy of brain metastatic disease: a systematic review & meta-analysis.BMC Cancer. 2021 Feb 16;21(1):167. doi: 10.1186/s12885-021-07889-3. BMC Cancer. 2021. PMID: 33593308 Free PMC article.
-
Comparison of WBRT alone, SRS alone, and their combination in the treatment of one or more brain metastases: Review and meta-analysis.Tumour Biol. 2017 Jul;39(7):1010428317702903. doi: 10.1177/1010428317702903. Tumour Biol. 2017. PMID: 28675121 Review.
Cited by
-
Comparison of a new MR rapid wash-out map with MR perfusion in brain tumors.BMC Cancer. 2024 Sep 12;24(1):1139. doi: 10.1186/s12885-024-12909-z. BMC Cancer. 2024. PMID: 39267002 Free PMC article.
-
Delayed Contrast-enhanced MRI Distinguishes Tumor from Radiation Treatment Effect.Radiol Imaging Cancer. 2025 May;7(3):e240388. doi: 10.1148/rycan.240388. Radiol Imaging Cancer. 2025. PMID: 40214516 Free PMC article. No abstract available.
-
Histopathological correlation of brain tumor recurrence vs. radiation effect post-radiosurgery as detected by MRI contrast clearance analysis: a validation study.J Neurooncol. 2024 Jul;168(3):547-553. doi: 10.1007/s11060-024-04697-0. Epub 2024 May 15. J Neurooncol. 2024. PMID: 38748050
-
Contrast Clearance Analysis (CCA) to Assess Viable Tumour following Stereotactic Radiosurgery (SRS) to Brain Metastasis in Non-Small Cell Lung Cancer (NSCLC).Cancers (Basel). 2024 Mar 20;16(6):1218. doi: 10.3390/cancers16061218. Cancers (Basel). 2024. PMID: 38539550 Free PMC article.
-
The value of stereotactic biopsy of primary and recurrent brain metastases in the era of precision medicine.Front Oncol. 2022 Dec 20;12:1014711. doi: 10.3389/fonc.2022.1014711. eCollection 2022. Front Oncol. 2022. PMID: 36605448 Free PMC article.
References
-
- Gerstner E.R., McNamara M.B., Norden A.D., Lafrankie D., Wen P.Y. Effect of adding temozolomide to radiation therapy on the incidence of pseudo-progression. J Neurooncol. 2009;94:97–101. - PubMed
-
- Wiggenraad R., Bos P., Verbeek-de Kanter A., et al. Pseudo-progression after stereotactic radiotherapy of brain metastases: lesion analysis using MRI cine-loops. J Neurooncol. 2014;119:437–443. - PubMed
-
- Bodensohn R., Hadi I., Fleischmann D.F., et al. Bevacizumab as a treatment option for radiation necrosis after cranial radiation therapy: a retrospective monocentric analysis. Strahlenther Onkol. 2020;196:70–76. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
