

Masquerade presentation of acute type B aortic dissection as isolated acute limb ischaemia treated with endovascular fenestration with angioplasty: A case report
- PMID: 35248883
- PMCID: PMC8898891
- DOI: 10.1016/j.ijscr.2022.106857
Masquerade presentation of acute type B aortic dissection as isolated acute limb ischaemia treated with endovascular fenestration with angioplasty: A case report
Abstract
Introduction and importance: Masquerade presentation of acute type B aortic dissections (TBAD) as acute limb ischaemia (ALI) is rare. Holistic clinical assessment, preferably with the help of scoring systems and timely computer tomographic angiogram (CTA), is needed for early diagnosis. Acute TBAD and its complications are increasingly treated with endovascular therapies.
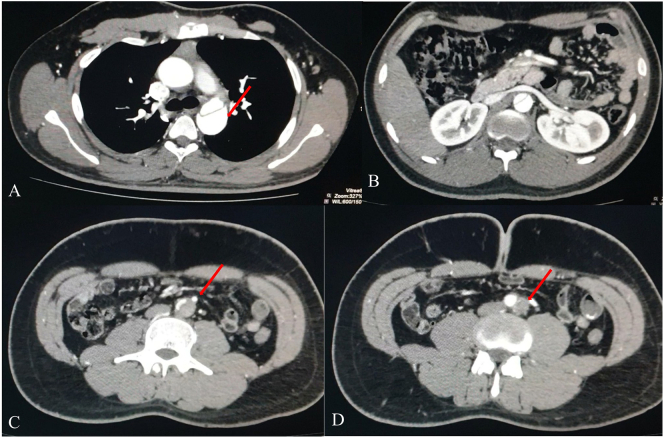
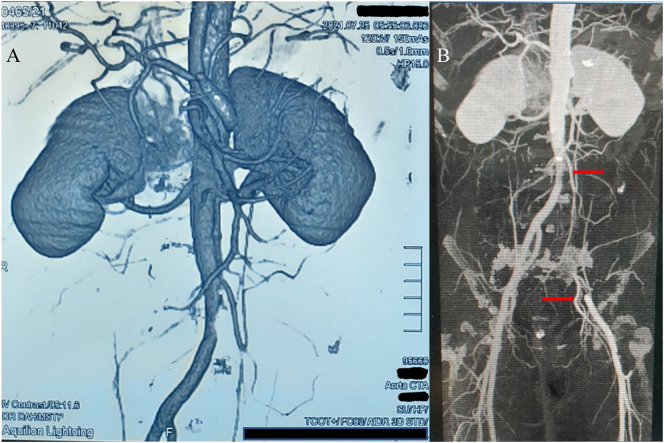
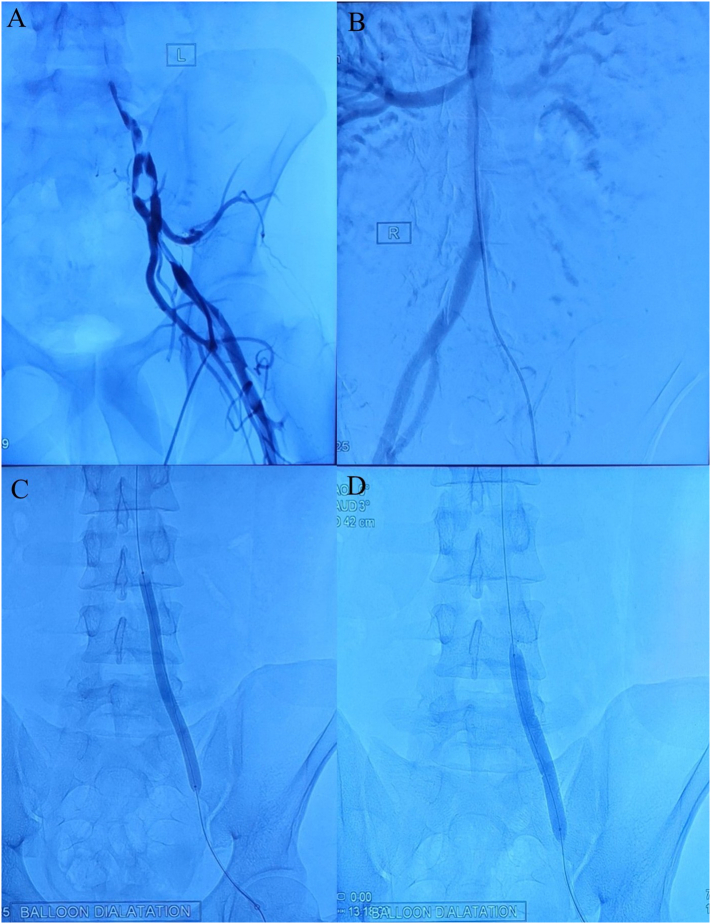
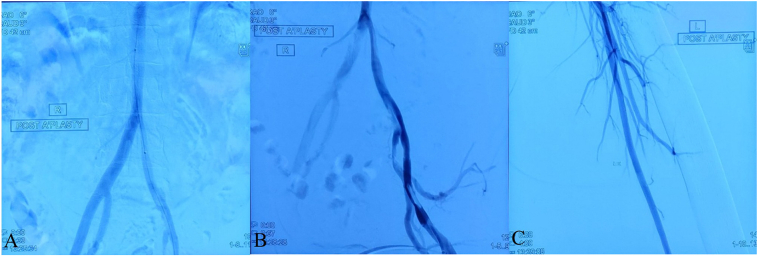
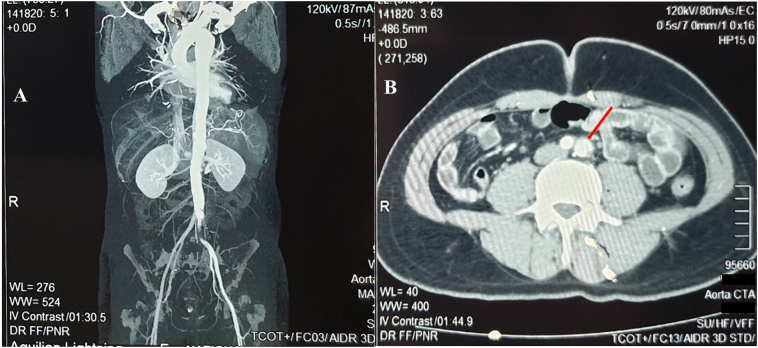
Case presentation: A 21-year-old male with poorly controlled essential hypertension was admitted with prominent clinical features of ALI. No clinical pointers of a TBAD were present. Doppler ultrasound revealed an arterial occlusive pattern, and an urgent surgical embolectomy was performed. On failure to retrieve any thrombi, a CTA was performed, and diagnosis of TBAD complicated with ALI was made. The limb was revascularised with guidewire directed aortic fenestration with angioplasty. TBAD was managed conservatively.
Clinical discussion: We report a case of acute TBAD presented as isolated ALI, which was initially diagnosed and treated as an ALI unrelated to aortic dissection. TBAD with typical or atypical clinical features presented with ALI as a malperfusion syndrome is not uncommon. However, masquerade presentations of TBAD as ALI are rare in the literature. Endovascular fenestration with or without stenting has fewer neurological complications and long-term mortality than thoracic endovascular aortic repair (TEVAR). Moreover, they become convenient in resource-poor settings without dedicated aortic centres.
Conclusion: Masquerade presentation of TBAD should be recognised in the differential diagnosis of ALI. Timely CTA would prevent unnecessary interventions and help diagnose TBAD complicated with ALI. Despite their availability, outcomes will depend on proper patient selection for endovascular, surgical, and TEVAR options.
Keywords: Acute limb ischaemia; Acute type B aortic dissection; Angioplasty; Case report; Endovascular fenestration; Malperfusion syndrome.
Copyright © 2022 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
None declared.
Figures
Similar articles
-
Management of acute type B aortic dissections and acute limb ischemia.J Cardiovasc Surg (Torino). 2011 Aug;52(4):507-17. J Cardiovasc Surg (Torino). 2011. PMID: 21792158 Review.
-
Surgical and endovascular repair for type B aortic dissections with mesenteric malperfusion syndrome: A systematic review of in-hospital mortality.JTCVS Open. 2022 Aug 8;12:37-50. doi: 10.1016/j.xjon.2022.07.012. eCollection 2022 Dec. JTCVS Open. 2022. PMID: 36590716 Free PMC article.
-
Thoracic Endovascular Aortic Repair (TEVAR) First in Patients with Lower Limb Ischemia in Complicated Type B Aortic Dissection: Clinical Outcome and Morphology.J Clin Med. 2022 Jul 17;11(14):4154. doi: 10.3390/jcm11144154. J Clin Med. 2022. PMID: 35887918 Free PMC article.
-
Lower limb malperfusion in type B aortic dissection: a systematic review.Ann Cardiothorac Surg. 2014 Jul;3(4):351-67. doi: 10.3978/j.issn.2225-319X.2014.07.05. Ann Cardiothorac Surg. 2014. PMID: 25133098 Free PMC article. Review.
-
Five-Year Results of Aortic Remodeling for Acute, Subacute, and Chronic Type B Aortic Dissection Following Endovascular Repair.Front Cardiovasc Med. 2022 May 17;9:847368. doi: 10.3389/fcvm.2022.847368. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35656393 Free PMC article.
References
-
- Clouse W., Hallett J., Schaff H., Spittell P., Rowland C., Ilstrup D., et al. Acute aortic dissection: population-based incidence compared with degenerative aortic aneurysm rupture. Mayo Clin. Proc. 2004 Mar;1(79):176–180. - PubMed
-
- Evangelista A., Isselbacher E.M., Bossone E., Gleason T.G., Di Eusanio M., Sechtem U., et al. Insights from the international registry of acute aortic dissection: a 20-year experience of collaborative clinical research. Circulation. 2018;137(17):1846–1860. - PubMed
-
- Cerneviciute R., Bicknell C.D. Acute type B aortic dissection. Surgery (United Kingdom) 2021;39(5):275–282. doi: 10.1016/j.mpsur.2021.03.007. [Internet] Available from. - DOI
-
- Agha R.A., Franchi T., Sohrabi C., Mathew G., Kerwan A., Thoma A., et al. The SCARE 2020 guideline: updating consensus Surgical CAse REport (SCARE) guidelines. Int. J. Surg. 2020;84:226–230. - PubMed
LinkOut - more resources
Full Text Sources
