

Beyond 10-Year Risk: A Cost-Effectiveness Analysis of Statins for the Primary Prevention of Cardiovascular Disease
- PMID: 35249370
- PMCID: PMC9022692
- DOI: 10.1161/CIRCULATIONAHA.121.057631
Beyond 10-Year Risk: A Cost-Effectiveness Analysis of Statins for the Primary Prevention of Cardiovascular Disease
Abstract
Background: Cholesterol guidelines typically prioritize primary prevention statin therapy on the basis of 10-year risk of cardiovascular disease. The advent of generic pricing may justify expansion of statin eligibility. Moreover, 10-year risk may not be the optimal approach for statin prioritization. We estimated the cost-effectiveness of expanding preventive statin eligibility and evaluated novel approaches to prioritization from a Scottish health sector perspective.
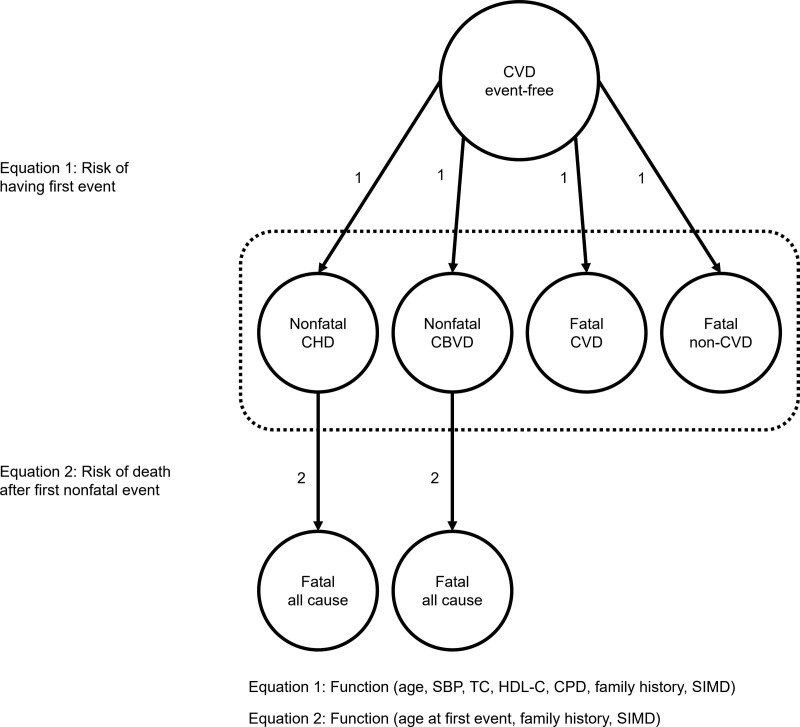
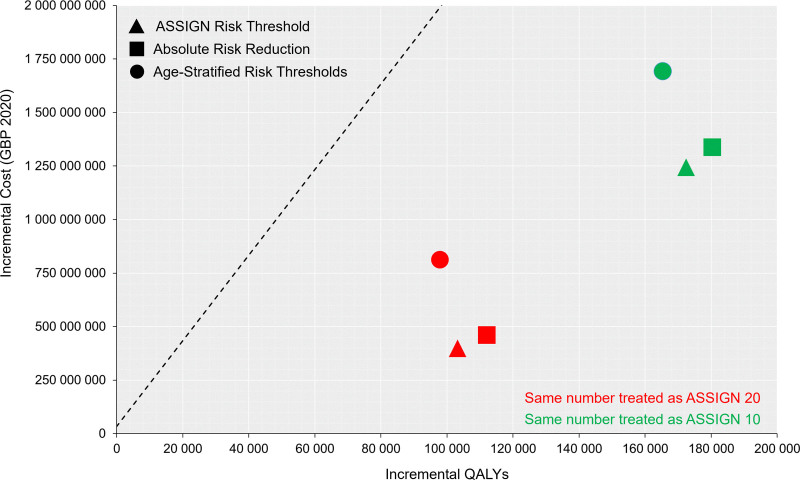
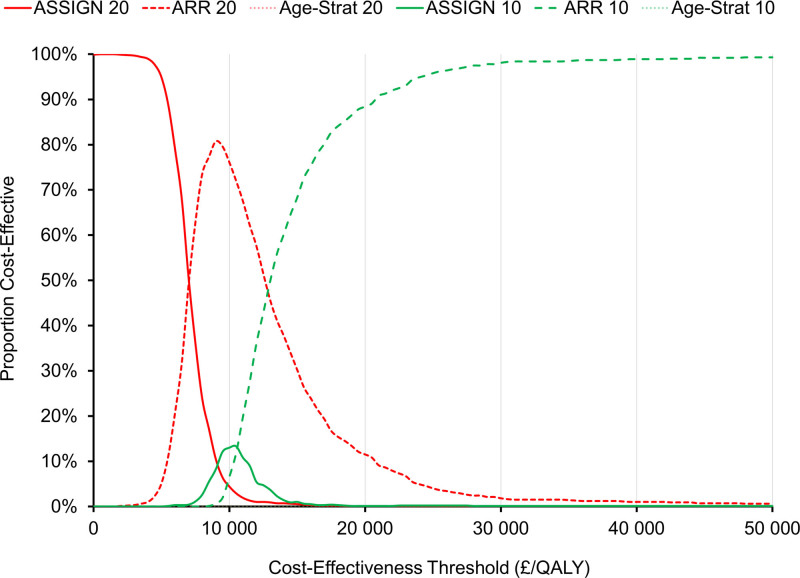
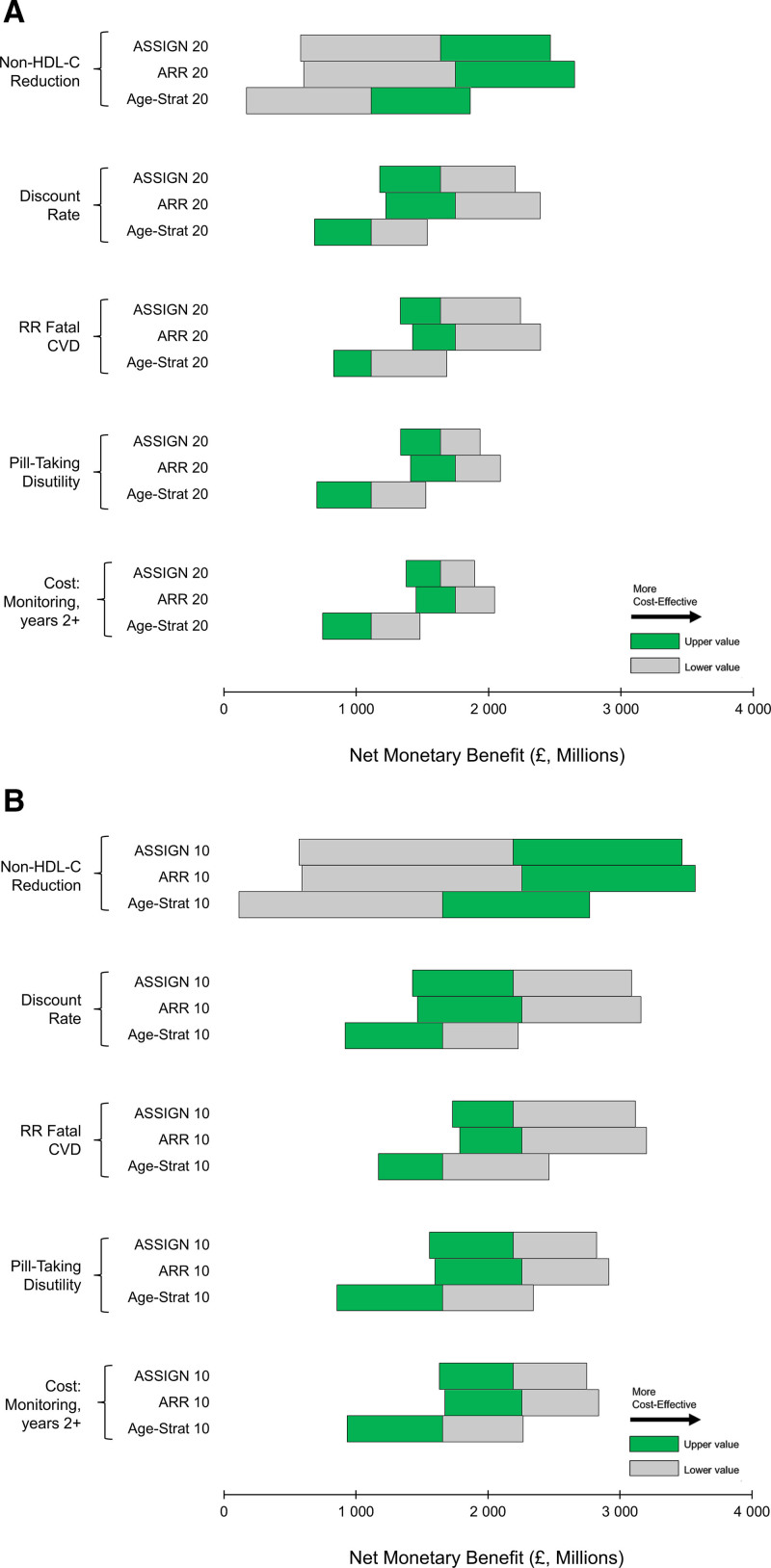
Methods: A computer simulation model predicted long-term health and cost outcomes in Scottish adults ≥40 years of age. Epidemiologic analysis was completed using the Scottish Heart Health Extended Cohort, Scottish Morbidity Records, and National Records of Scotland. A simulation cohort was constructed with data from the Scottish Health Survey 2011 and contemporary population estimates. Treatment and cost inputs were derived from published literature and health service cost data. The main outcome measure was the lifetime incremental cost-effectiveness ratio, evaluated as cost (2020 GBP) per quality-adjusted life-year (QALY) gained. Three approaches to statin prioritization were analyzed: 10-year risk scoring using the ASSIGN score, age-stratified risk thresholds to increase treatment rates in younger individuals, and absolute risk reduction (ARR)-guided therapy to increase treatment rates in individuals with elevated cholesterol levels. For each approach, 2 policies were considered: treating the same number of individuals as those with an ASSIGN score ≥20% (age-stratified risk threshold 20, ARR 20) and treating the same number of individuals as those with an ASSIGN score ≥10% (age-stratified risk threshold 10, ARR 10).
Results: Compared with an ASSIGN score ≥20%, reducing the risk threshold for statin initiation to 10% expanded eligibility from 804 000 (32% of adults ≥40 years of age without CVD) to 1 445 500 individuals (58%). This policy would be cost-effective (incremental cost-effectiveness ratio, £12 300/QALY [95% CI, £7690/QALY-£26 500/QALY]). Incremental to an ASSIGN score ≥20%, ARR 20 produced ≈8800 QALYs and was cost-effective (£7050/QALY [95% CI, £4560/QALY-£10 700/QALY]). Incremental to an ASSIGN score ≥10%, ARR 10 produced ≈7950 QALYs and was cost-effective (£11 700/QALY [95% CI, £9250/QALY-£16 900/QALY]). Both age-stratified risk threshold strategies were dominated (ie, more expensive and less effective than alternative treatment strategies).
Conclusions: Generic pricing has rendered preventive statin therapy cost-effective for many adults. ARR-guided therapy is more effective than 10-year risk scoring and is cost-effective.
Keywords: cardiovascular diseases; cholesterol; hydroxymethylglutaryl-CoA reductase; risk.
Figures
Comment in
-
Commentary: Beyond 10-year risk: A cost-effectiveness analysis of statins for the primary prevention of cardiovascular disease.Front Cardiovasc Med. 2022 Jul 22;9:916695. doi: 10.3389/fcvm.2022.916695. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35935628 Free PMC article. No abstract available.
References
-
- Roth GA, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, Abbastabar H, Abd-Allah F, Abdela J, Abdelalim A, et al. . Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1736–1788. doi: 10.1016/S0140-6736(18)32203-7 - PMC - PubMed
-
- Office for National Statistics. Deaths registered in England and Wales: 2019. Published 2020. Accessed October 12, 2021. https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarri...
-
- National Records of Scotland. Vital Events Reference Tables 2018. Published 2019. Accessed November 19, 2019. https://webarchive.nrscotland.gov.uk/20210314054215/https://www.nrscotla...
-
- National Clinical Guideline Centre. Lipid modification: cardiovascular risk assessment and the modification of blood lipids for the primary and secondary prevention of cardiovascular disease. Published 2014. Accessed March 23, 2021. http://www.ncbi.nlm.nih.gov/books/NBK248067/ - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
