

CT Imaging Features in Acute Invasive Fungal Rhinosinusitis- Recalling the Oblivion in the COVID Era
- PMID: 35249797
- PMCID: PMC8820107
- DOI: 10.1067/j.cpradiol.2022.02.001
CT Imaging Features in Acute Invasive Fungal Rhinosinusitis- Recalling the Oblivion in the COVID Era
Abstract
Objective: Recent pandemic of COVID19 infection has witnessed a re-emergence of invasive fungal sinusitis especially of the Mucor species, which has been a rare entity in the pre covid era. Covid associated mucormycosis (CAM) is one of the dreaded and fatal complications which has surfaced up and early diagnosis is critical for management and survival .It is identified to affect both subset of patients, those with active COVID-19 infection and those who have recovered from the disease in the last 4-6 weeks. Imaging features suggestive of early invasion with supportive imaging examples and relevance of these findings in clinical decision making is presented.
Methods: This paper reviews the various imaging signs of early invasion in CAM A comprehensive checklist for clinically relevant and quick reporting is also presented.
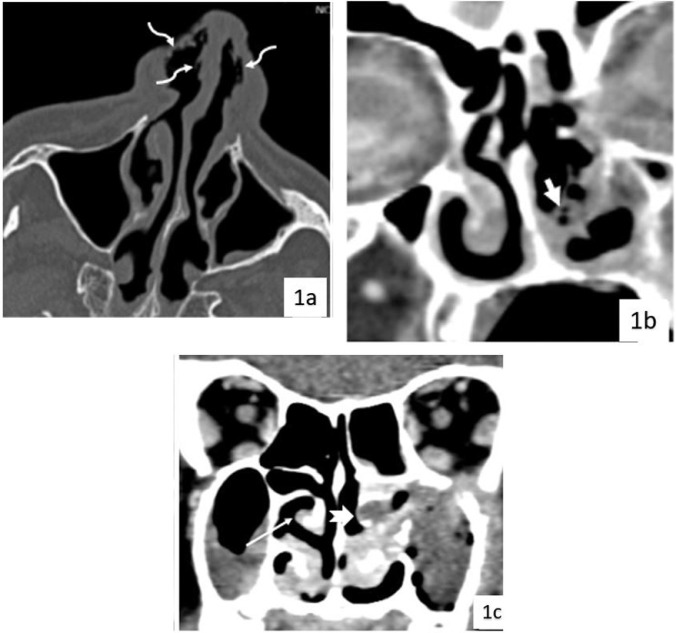
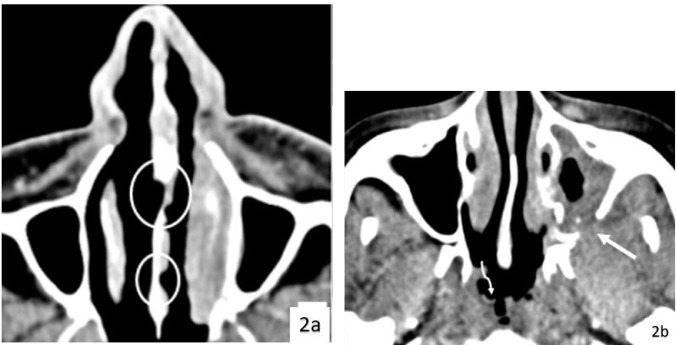
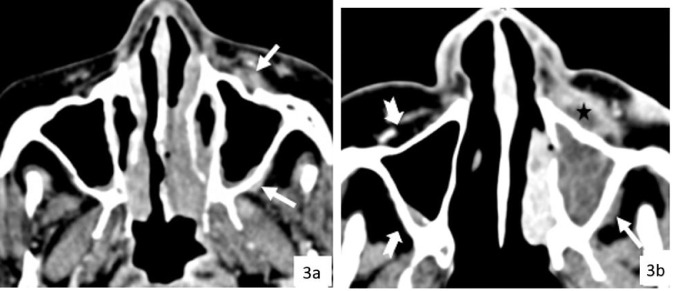
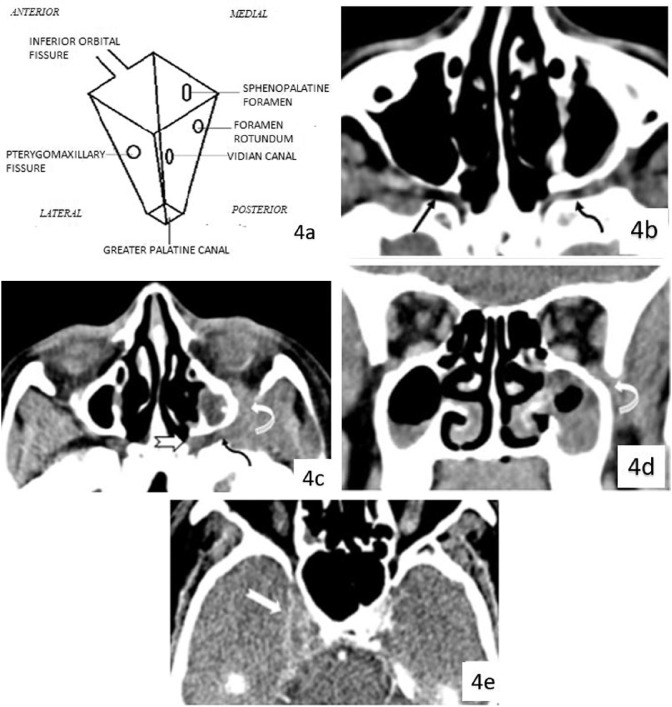
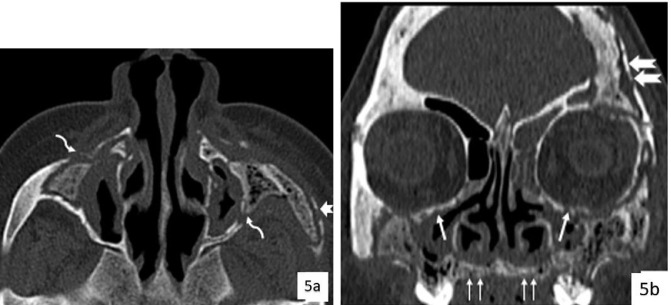
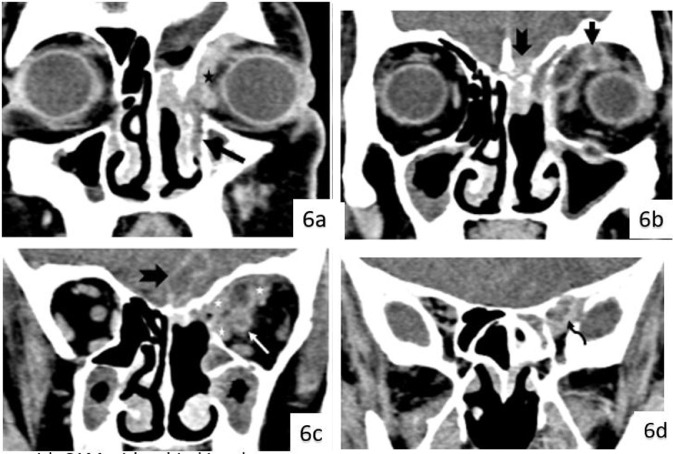
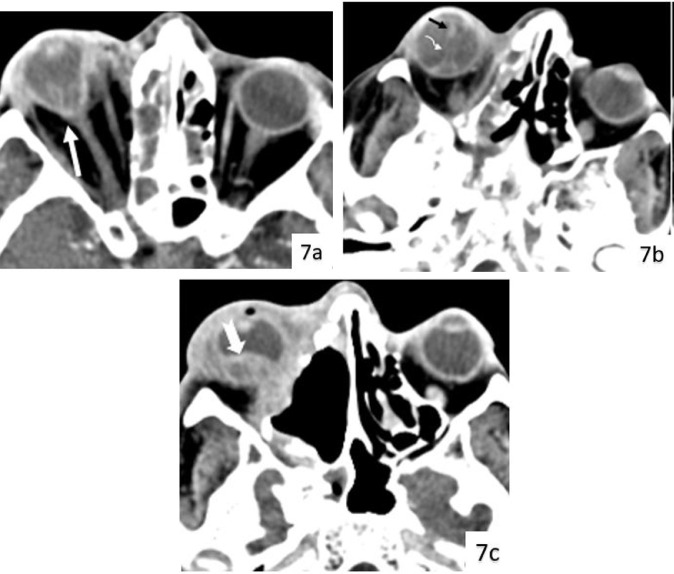
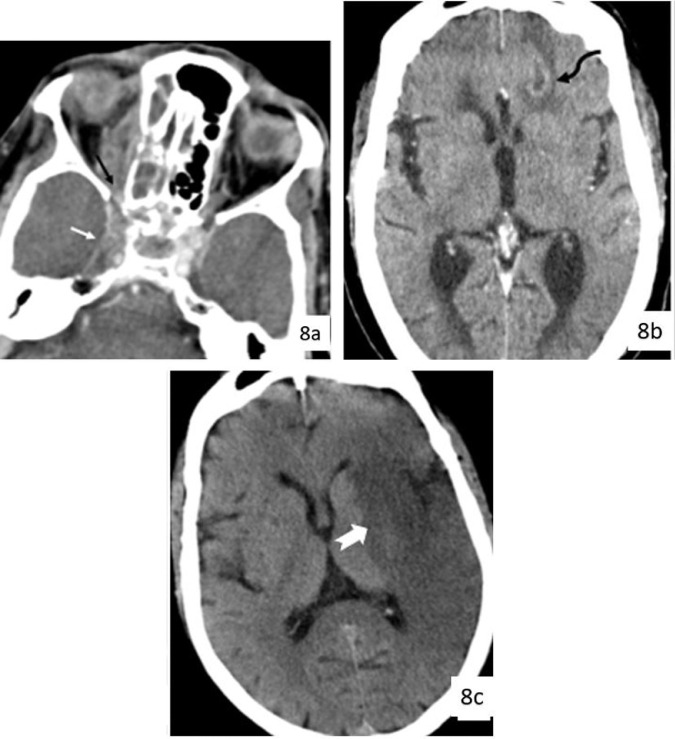
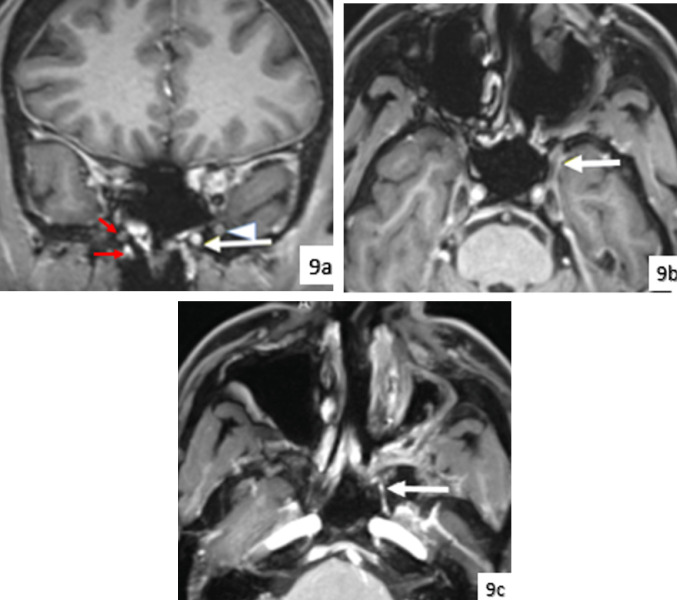
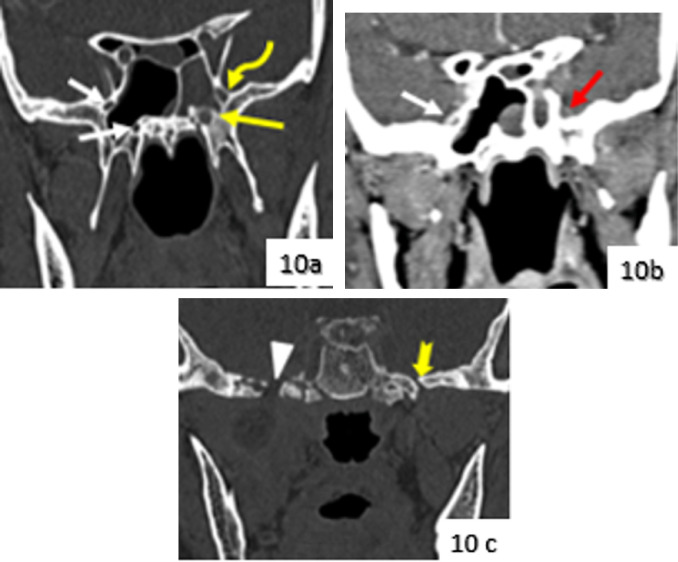
Results: Emphysematous or ulcerative mucosal changes in the nasal cavity is an early imaging feature of CAM. Periantral soft tissue and soft tissue within the pterygopalatine fossa are important imaging signs to indicate extrasinus invasion. Disease within pterygopalatine fossa may lead to multidirectional spread and is an important check site. These findings are seen even in absence of bony erosions owing to the neurovascular spread of disease. Intra orbital and intracranial extensions were found to be fairly common and must be sought for.
Conclusion: The knowledge of early subtle signs of CAM on imaging can aid in prompt diagnosis of this fatal entity in the pertinent clinical setting. Imaging signs of spread of disease and delineation of its extent as inferred from CT imaging aids in prognosis and appropriate surgical management.
Copyright © 2022 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Computed tomographic findings in patients with invasive fungal sinusitis.Arch Otolaryngol Head Neck Surg. 2003 Feb;129(2):236-40. doi: 10.1001/archotol.129.2.236. Arch Otolaryngol Head Neck Surg. 2003. PMID: 12578456
-
Magnetic resonance imaging in COVID-19-associated acute invasive fungal rhinosinusitis - Diagnosis and beyond.J Clin Imaging Sci. 2023 Aug 9;13:23. doi: 10.25259/JCIS_46_2023. eCollection 2023. J Clin Imaging Sci. 2023. PMID: 37680251 Free PMC article.
-
The Algorithmic Role of Critical Radiographic Features in the Treatment of Angioinvasive Fungal Sinusitis.Ophthalmic Plast Reconstr Surg. 2025 Jan-Feb 01;41(1):1-7. doi: 10.1097/IOP.0000000000002783. Epub 2024 Sep 6. Ophthalmic Plast Reconstr Surg. 2025. PMID: 39240228 Review.
-
Imaging Features of Invasive Fungal Rhinosinusitis: A Systematic Review.Can Assoc Radiol J. 2024 Aug;75(3):601-608. doi: 10.1177/08465371241227424. Epub 2024 Feb 12. Can Assoc Radiol J. 2024. PMID: 38344986
-
Revisiting rhino-orbito-cerebral acute invasive fungal sinusitis in the era of COVID-19: pictorial review.Emerg Radiol. 2021 Dec;28(6):1063-1072. doi: 10.1007/s10140-021-01980-9. Epub 2021 Aug 31. Emerg Radiol. 2021. PMID: 34463864 Free PMC article. Review.
Cited by
-
Presumptive Rhino-Orbital Mucormycosis Secondary to Corticosteroid Therapy in a Diabetic Patient With COVID-19 Infection.Cureus. 2023 Feb 19;15(2):e35199. doi: 10.7759/cureus.35199. eCollection 2023 Feb. Cureus. 2023. PMID: 36968851 Free PMC article.
-
Is low dose of liposomal amphotericin B effective in management of acute invasive fungal rhinosinusitis? Our conclusions from Al-Mowassat University Hospital, Syria: a prospective observational study.BMC Infect Dis. 2023 Mar 31;23(1):196. doi: 10.1186/s12879-023-08177-0. BMC Infect Dis. 2023. PMID: 37004006 Free PMC article.
-
MR imaging spectrum in COVID associated Rhino-Orbito-Cerebral mucormycosis with special emphasis on intracranial disease and impact on patient prognosis.Eur J Radiol. 2022 Jul;152:110341. doi: 10.1016/j.ejrad.2022.110341. Epub 2022 May 6. Eur J Radiol. 2022. PMID: 35569303 Free PMC article. Review.
-
Epidemiology, pathogenesis, clinical characteristics, and treatment of mucormycosis: a review.Ann Med. 2024 Dec;56(1):2396570. doi: 10.1080/07853890.2024.2396570. Epub 2024 Sep 2. Ann Med. 2024. PMID: 39221718 Free PMC article. Review.
References
-
- Franquet T, Giménez A, Hidalgo A. Imaging of opportunistic fungal infections in immunocompromised patient. Eur J Radiol. 2004;51:130–138. - PubMed
-
- Süslü A, Öğretmenoğlu O, Süslü N, et al. Acute invasive fungal rhinosinusitis: our experience with 19 patients. Eur Arch Otorhinolaryngol. 2009;266:77–82. - PubMed
-
- Valera F, Lago T, Tamashiro E, et al. Prognosis of acute invasive fungal rhinosinusitis related to underlying disease. Int J Infect Dis. 2011;15:e841–e844. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
