

Health Resource Use in Survivors of Pediatric Septic Shock in the United States
- PMID: 35250001
- PMCID: PMC9203867
- DOI: 10.1097/PCC.0000000000002932
Health Resource Use in Survivors of Pediatric Septic Shock in the United States
Abstract
Objectives: To evaluate postdischarge health resource use in pediatric survivors of septic shock and determine patient and hospitalization factors associated with health resource use.
Design: Secondary analyses of a multicenter prospective observational cohort study.
Setting: Twelve academic PICUs.
Patients: Children greater than or equal to 1 month and less than 18 years old hospitalized for community-acquired septic shock who survived to 1 year.
Interventions: None.
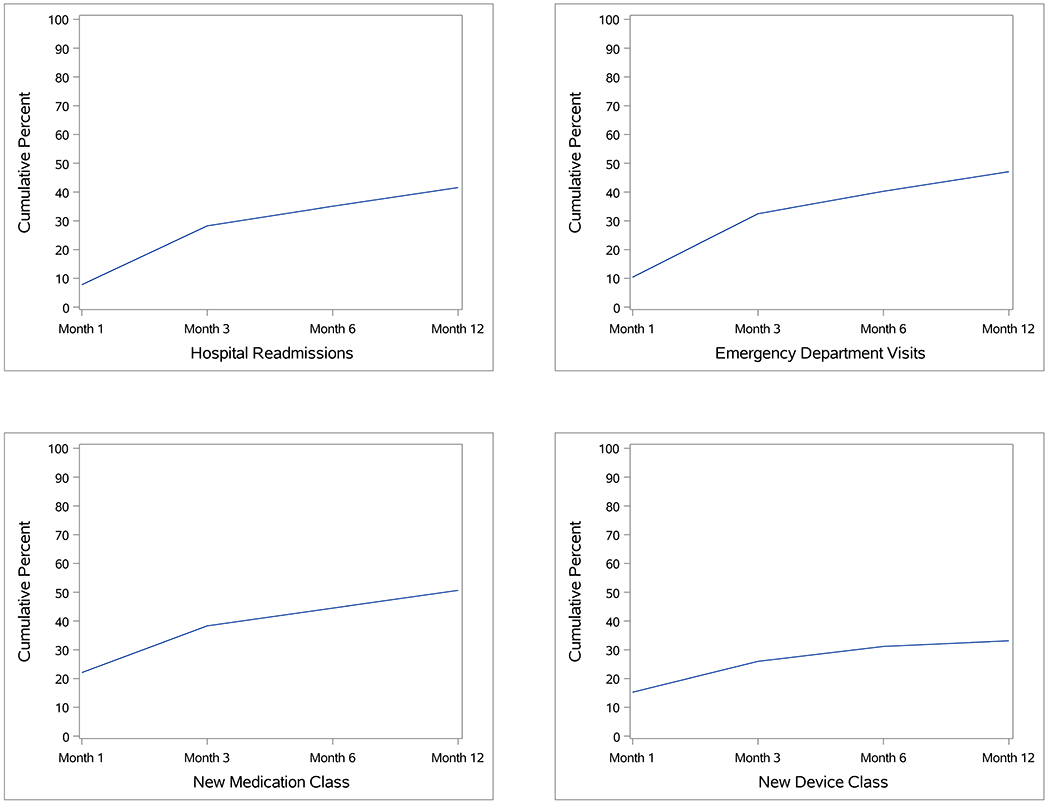
Measurements and main results: For 308/338 patients (91%) with baseline and greater than or equal to one postdischarge survey, we evaluated readmission, emergency department (ED) visits, new medication class, and new device class use during the year after sepsis. Using negative binomial regression with bidirectional stepwise selection, we identified factors associated with each outcome. Median age was 7 years (interquartile range, 2-13), 157 (51%) had a chronic condition, and nearly all patients had insurance (private [n = 135; 44%] or government [n = 157; 51%]). During the year after sepsis, 128 patients (42%) were readmitted, 145 (47%) had an ED visit, 156 (51%) started a new medication class, and 102 (33%) instituted a new device class. Having a complex chronic condition was independently associated with readmission and ED visit. Documented infection and higher sum of Pediatric Logistic Organ Dysfunction--2 hematologic score were associated with readmission, whereas younger age and having a noncomplex chronic condition were associated with ED visit. Factors associated with new medication class use were private insurance, neurologic insult, and longer PICU stays. Factors associated with new device class use were preadmission chemotherapy or radiotherapy, presepsis Functional Status Scale score, and ventilation duration greater than or equal to 10 days. Of patients who had a new medication or device class, most had a readmission (56% and 61%) or ED visit (62% and 67%).
Conclusions: Children with septic shock represent a high-risk cohort with high-resource needs after discharge. Interventions and targeted outcomes to mitigate postdischarge resource use may differ based on patients' preexisting conditions.
Copyright © 2022 by the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies.
Conflict of interest statement
Dr. Maddux’s institution received funding from the National Institute of Child Health and Human Development (NICHD) (K23HD096018) and the Francis Family Foundation. Drs. Maddux, Zimmerman, Banks, Reeder, Meert, Berg, Sapru, Carcillo, Newth, and Mourani received support for article research from the National Institutes of Health (NIH). Drs. Zimmerman’s, Banks’, and Carcillo’s institution received funding from the NICHD. Dr. Zimmerman’s institution received funding from Immunexpress; he received funding from Elsevier Publishing. Dr. Banks disclosed government work. Drs. Reeder’s, Meert’s, Berg’s, Sapru’s, Newth’s, and Mourani’s institutions received funding from the NIH. Dr. Czaja disclosed that she is a member of the critical care subboard for the American Board of Pediatrics. Dr. Carcillo’s institution received funding from the National Institute of General Medical Sciences. Dr. Newth received funding from Philips Research North America and Nihon Kohden. Dr. Mourani received funding from the NICHD (UG1HD083171). Dr. Quasney has disclosed that he does not have any potential conflicts of interest.
Figures
References
-
- Ruth A, McCracken CE, Fortenberry JD, et al. Pediatric severe sepsis: current trends and outcomes from the Pediatric Health Information Systems database. Pediatr Crit Care Med. 2014. Nov;15(9):828–38. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 GM108618/GM/NIGMS NIH HHS/United States
- R03 HD104001/HD/NICHD NIH HHS/United States
- RL1 HD107777/HD/NICHD NIH HHS/United States
- U10 HD050012/HD/NICHD NIH HHS/United States
- UG1 HD049983/HD/NICHD NIH HHS/United States
- RL1 HD107779/HD/NICHD NIH HHS/United States
- U10 HD049983/HD/NICHD NIH HHS/United States
- U10 HD063106/HD/NICHD NIH HHS/United States
- UG1 HD063108/HD/NICHD NIH HHS/United States
- RL1 HD107773/HD/NICHD NIH HHS/United States
- R01 HD073362/HD/NICHD NIH HHS/United States
- UG1 HD083171/HD/NICHD NIH HHS/United States
- U01 HD049934/HD/NICHD NIH HHS/United States
- UG1 HD049981/HD/NICHD NIH HHS/United States
- K23 HD096018/HD/NICHD NIH HHS/United States
- UG1 HD050096/HD/NICHD NIH HHS/United States
- UG1 HD083170/HD/NICHD NIH HHS/United States
- UG1 HD083166/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
