

Instrument Referral Criteria for PlusoptiX, SPOT and 2WIN Targeting 2021 AAPOS Guidelines
- PMID: 35250260
- PMCID: PMC8893268
- DOI: 10.2147/OPTH.S342666
Instrument Referral Criteria for PlusoptiX, SPOT and 2WIN Targeting 2021 AAPOS Guidelines
Erratum in
-
Erratum: Instrument Referral Criteria for PlusoptiX, SPOT and 2WIN Targeting 2021 AAPOS Guidelines [Corrigendum].Clin Ophthalmol. 2025 Apr 5;19:1215-1216. doi: 10.2147/OPTH.S531945. eCollection 2025. Clin Ophthalmol. 2025. PMID: 40213508 Free PMC article.
Abstract
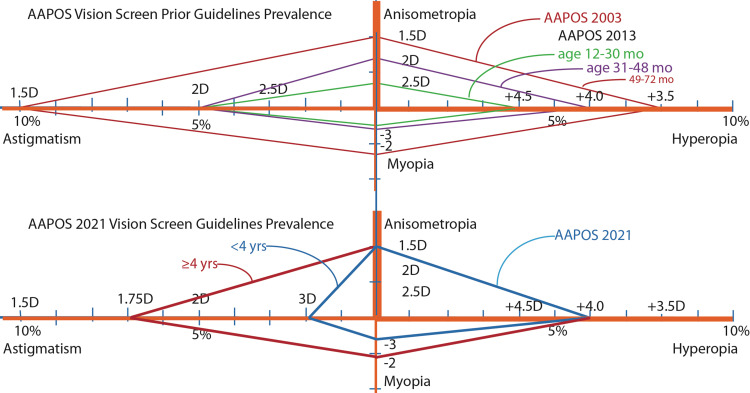
Background: The American Association for Pediatric Ophthalmology and Strabismus (AAPOS) issued a 2021 update of Uniform Validation Guidelines for instrument-based pediatric vision screeners. With each update it is important for each manufacturer to update the Instrument Referral Criteria (IRC) programed into their devices in order to optimize sensitivity and specificity to detect AAPOS criteria.
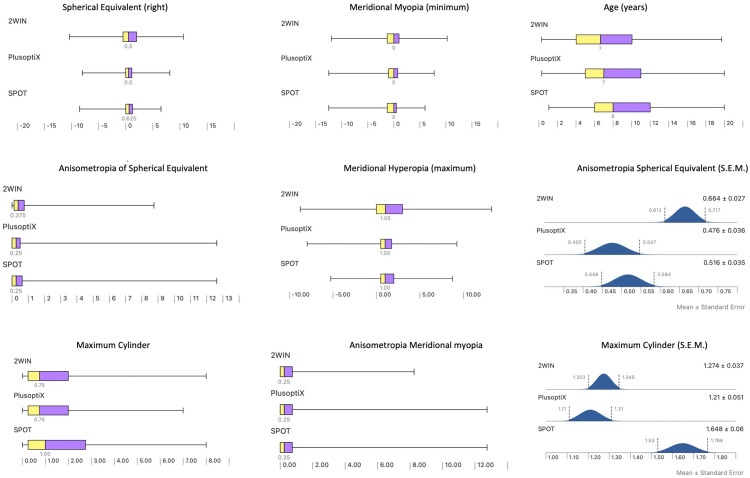
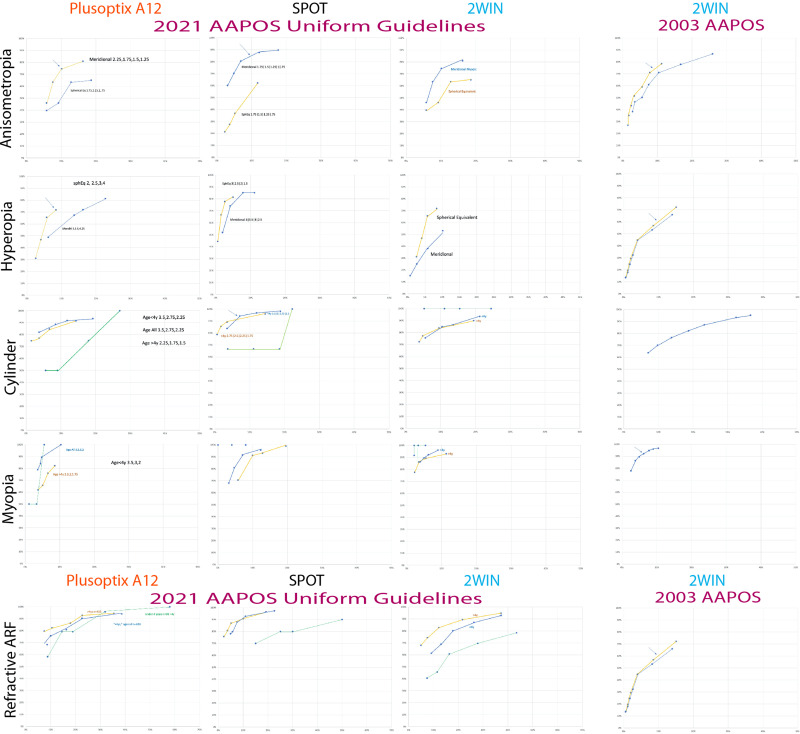
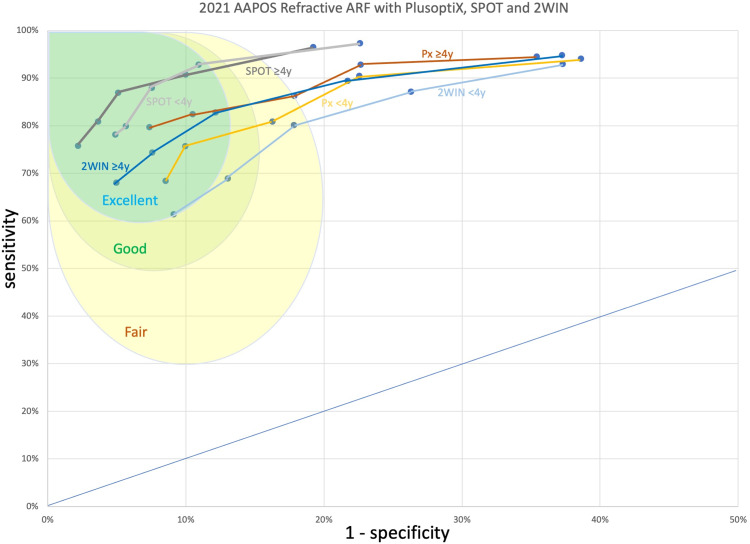
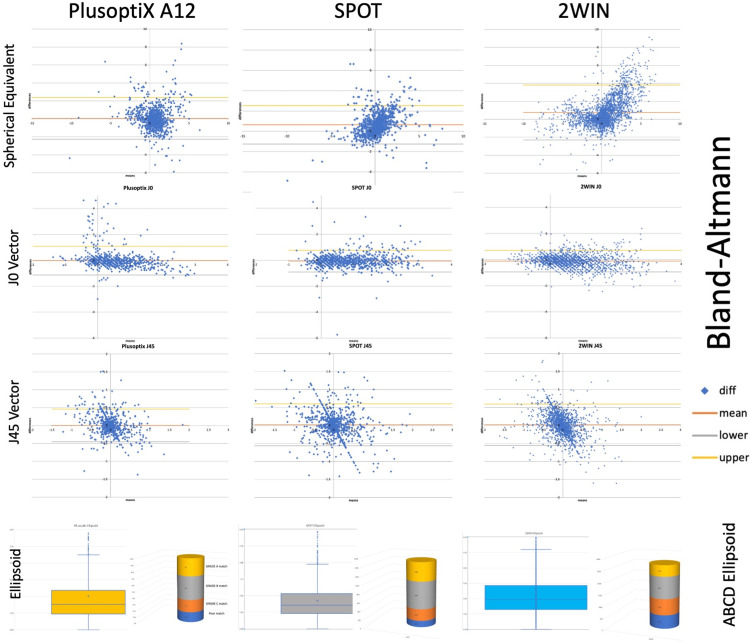
Methods: De-identified data comparing photoscreening with simultaneous confirmatory examinations constituted separate cohorts for the development of IRC via receiver operating characteristic (ROC) curves. The refractions of the devices were also compared.
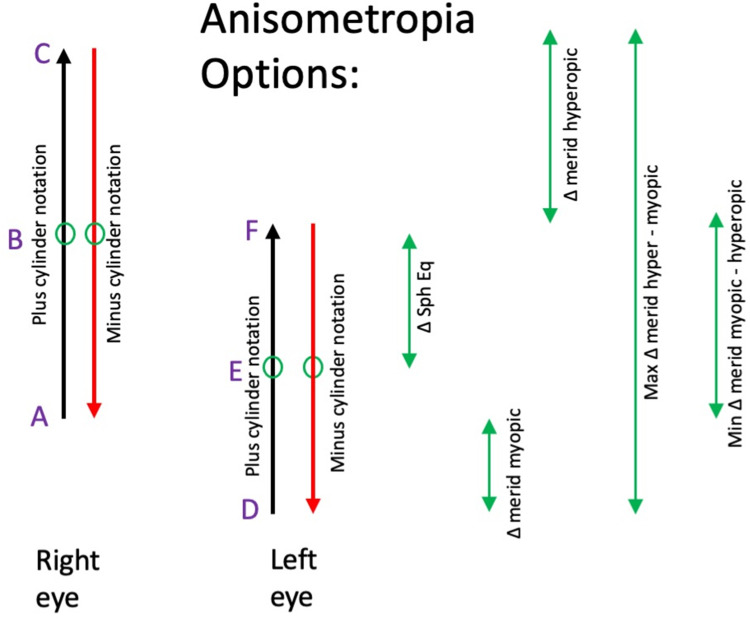
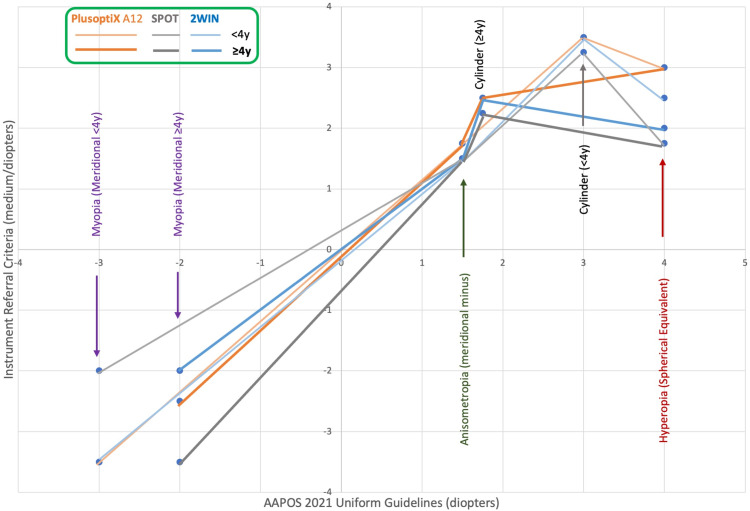
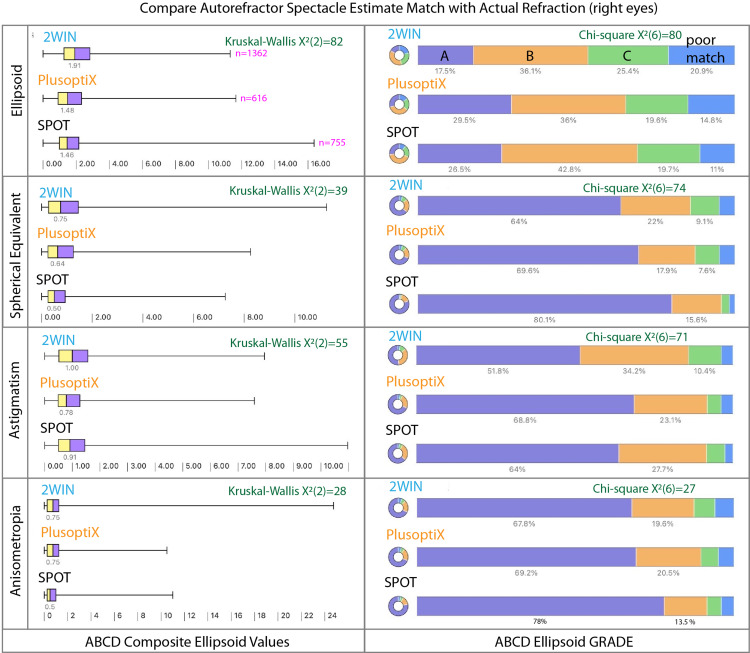
Results: This study defines three sets of refractive IRC (Sensitive, Medium, and Specific) for three leading infrared photoscreening devices, PlusoptiX A12, Welch-Allyn SPOT, and Adaptica 2WIN for children < 4 and ≥ 4 years in order to better target the 2021 AAPOS guidelines. The cohorts were similar but the SPOT group (n=755, mean age 9) was older with more astigmatism and the 2WIN (n=1362, mean age 7) was younger with more hyperopia and anisometropia compared to the cohort for PlusoptiX A12 (n=616, mean age 8). The age-based, medium magnitude IRC for anisometropia, hyperopia, astigmatism and myopia for SPOT were: <4y: 1.5, 1.75, 3.25, 3.5 and ≥4y: 1.5, 1.75, 2.25, 2.0; for PlusoptiX: <4y: 1.75, 3.0, 3.5, 3.5 and ≥4y: 1.75, 3.0, 2.5, 2.5; and for 2WIN: <4y: 1.75, 2.5, 3.5, 3.5 and ≥4y: 1.5, 2.0, 2.5, 2.0. The mean ABCD ellipsoid spectacle matches differed; SPOT: 1.8±1.3 (better) versus PlusoptiX: 1.9±1.6 and 2WIN: 2.2±1.4 (p<0.001).
Conclusion: The 2021 AAPOS exam guidelines foster early specificity before age 4 and sensitivity after age 4. These evidence-based IRC for current SPOT, PlusoptiX, and 2WIN photoscreeners should allow device manufacturers the data necessary to adjust their device IRC to maximize specificity, sensitivity or a medium between the two. This paper provides practical suggestions for better validation. Improved early screening combined with thorough treatment should reduce life-long vision impairment due to amblyopia.
Keywords: amblyopia; amblyopia risk factors; infrared autorefractor; refraction; vision screening; visually significant refractive errors.
© 2022 Arnold et al.
Conflict of interest statement
Dr. Arnold is President of Glacier Medical software that markets cloud-based ROP-Check software. Dr. Arnold is President of PDI Check that developed a vision screening game for Nintendo 3DS. Dr Arnold is an investigator and protocol developer for PEDIG. Dr. Arnold coordinates the Alaska Blind Child Discovery which has received discounted vision screen technology from several vendors. He is a non-paid member of advisory boards to PlusoptiX, GoCheck Kids, Adaptica, NovaSight, and iScreen. Robert Arnold also reports patent pending for autostereoscopic vision screening game to PDI check. Dr. Silbert is Founder of KinderSee a school-based eye clinic serving the children of Lancaster County PA, he serves on the Medical Advisory Board and holds stock options in GoCheck Kids. He is a consultant for Kaneka America and a speaker for Horizon Therapeutics. He is a co-founder and co-owner for remote amblyopia monitoring and treatment at Amblyopia Home. Heather Modjesky reports no conflicts of interest in this work.
Figures


References
-
- Wilson J, Junger G Principles and practice of screening for disease. Public Health paper No 34. World Health Organization; 1968.
-
- Silverstein E, Donahue SP. Preschool vision screening: where we have been and where we are going. Am J Ophthalmol. 2018;194:18–23. - PubMed
-
- Donahue S, Arnold R, Ruben JB. Preschool vision screening: what should we be detecting and how should we report it? Uniform guidelines for reporting results from studies of preschool vision screening. J AAPOS. 2003;7(5):314–316. - PubMed
-
- Donahue SP, Arthur B, Neely DE, Arnold RW, Silbert D, Ruben JB. Guidelines for automated preschool vision screening: a 10-year, evidence-based update. J AAPOS. 2013;17(1):4–8. - PubMed
LinkOut - more resources
Full Text Sources
