

Tumor Immune Microenvironment and Immunotherapy in Brain Metastasis From Non-Small Cell Lung Cancer
- PMID: 35251014
- PMCID: PMC8891382
- DOI: 10.3389/fimmu.2022.829451
Tumor Immune Microenvironment and Immunotherapy in Brain Metastasis From Non-Small Cell Lung Cancer
Abstract
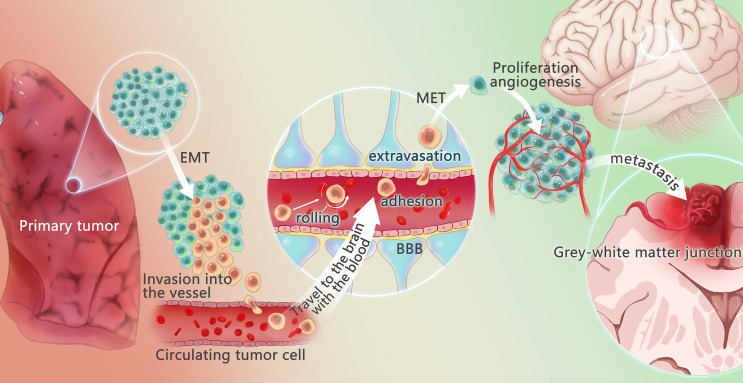
Brain metastasis (BM), a devastating complication of advanced malignancy, has a high incidence in non-small cell lung cancer (NSCLC). As novel systemic treatment drugs and improved, more sensitive imaging investigations are performed, more patients will be diagnosed with BM. However, the main treatment methods face a high risk of complications at present. Therefore, based on immunotherapy of tumor immune microenvironment has been proposed. The development of NSCLC and its BM is closely related to the tumor microenvironment, the surrounding microenvironment where tumor cells live. In the event of BM, the metastatic tumor microenvironment in BM is composed of extracellular matrix, tissue-resident cells that change with tumor colonization and blood-derived immune cells. Immune-related cells and chemicals in the NSCLC brain metastasis microenvironment are targeted by BM immunotherapy, with immune checkpoint inhibition therapy being the most important. Blocking cancer immunosuppression by targeting immune checkpoints provides a suitable strategy for immunotherapy in patients with advanced cancers. In the past few years, several therapeutic advances in immunotherapy have changed the outlook for the treatment of BM from NSCLC. According to emerging evidence, immunotherapy plays an essential role in treating BM, with a more significant safety profile than others. This article discusses recent advances in the biology of BM from NSCLC, reviews novel mechanisms in diverse tumor metastatic stages, and emphasizes the role of the tumor immune microenvironment in metastasis. In addition, clinical advances in immunotherapy for this disease are mentioned.
Keywords: BM; NSCLC; PD-1 inhibitor; PD-L1 inhibitor; cancer; immunotherapy.
Copyright © 2022 Wang, Chen, Wa, Ding, Yang, Liao, Tong and Xiao.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
The Emerging Role of Immune Checkpoint Blockade for the Treatment of Lung Cancer Brain Metastases.Clin Lung Cancer. 2024 Sep;25(6):483-501. doi: 10.1016/j.cllc.2024.06.004. Epub 2024 Jun 10. Clin Lung Cancer. 2024. PMID: 38991863 Review.
-
Immunotherapy in NSCLC patients with brain metastases. Understanding brain tumor microenvironment and dissecting outcomes from immune checkpoint blockade in the clinic.Cancer Treat Rev. 2020 Sep;89:102067. doi: 10.1016/j.ctrv.2020.102067. Epub 2020 Jul 7. Cancer Treat Rev. 2020. PMID: 32682248 Review.
-
Immunotherapy and the Tumor Microenvironment in Brain Metastases from Non-Small Cell Lung Cancer: Challenges and Future Directions.Curr Oncol. 2025 Mar 16;32(3):171. doi: 10.3390/curroncol32030171. Curr Oncol. 2025. PMID: 40136375 Free PMC article. Review.
-
Immune checkpoint inhibitors for brain metastases in non-small-cell lung cancer: from rationale to clinical application.Immunotherapy. 2021 Aug;13(12):1031-1051. doi: 10.2217/imt-2020-0262. Epub 2021 Jul 7. Immunotherapy. 2021. PMID: 34231370 Review.
-
Immunotherapy and brain metastasis in lung cancer: connecting bench side science to the clinic.Front Immunol. 2023 Oct 9;14:1221097. doi: 10.3389/fimmu.2023.1221097. eCollection 2023. Front Immunol. 2023. PMID: 37876939 Free PMC article. Review.
Cited by
-
Cinobufagin inhibits M2‑like tumor‑associated macrophage polarization to attenuate the invasion and migration of lung cancer cells.Int J Oncol. 2024 Nov;65(5):102. doi: 10.3892/ijo.2024.5690. Epub 2024 Sep 20. Int J Oncol. 2024. PMID: 39301639 Free PMC article.
-
Exploring the prognostic potential of m6A methylation regulators in low-grade glioma: implications for tumor microenvironment modulation.Eur J Med Res. 2024 Jan 3;29(1):19. doi: 10.1186/s40001-023-01621-6. Eur J Med Res. 2024. PMID: 38173044 Free PMC article.
-
Application of random survival forest to establish a nomogram combining clinlabomics-score and clinical data for predicting brain metastasis in primary lung cancer.Clin Transl Oncol. 2025 Apr;27(4):1472-1483. doi: 10.1007/s12094-024-03688-x. Epub 2024 Sep 3. Clin Transl Oncol. 2025. PMID: 39225959 Free PMC article.
-
Therapeutic efficacy of TMTP1-modified EVs in overcoming bone metastasis and immune resistance in PIK3CA mutant NSCLC.Cell Death Dis. 2025 May 6;16(1):367. doi: 10.1038/s41419-025-07685-y. Cell Death Dis. 2025. PMID: 40328748 Free PMC article.
-
Patient-Derived Lung Cancer "Sandwich Cultures" with a Preserved Tumor Microenvironment.Tissue Eng Part C Methods. 2024 Jan;30(1):27-37. doi: 10.1089/ten.TEC.2023.0199. Tissue Eng Part C Methods. 2024. PMID: 38115596 Free PMC article.
References
-
- Fitzmaurice C, Abate D, Abbasi N, Abbastabar H, Abd-Allah F, Abdel-Rahman O, et al. . Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2017: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol (2019) 5(12):1749–68. doi: 10.1001/jamaoncol.2019.2996 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous