

Case Report: Myxedema Coma Caused by Immunoglobulin A Vasculitis in a Patient With Severe Hypothyroidism
- PMID: 35251034
- PMCID: PMC8895252
- DOI: 10.3389/fimmu.2022.838739
Case Report: Myxedema Coma Caused by Immunoglobulin A Vasculitis in a Patient With Severe Hypothyroidism
Abstract
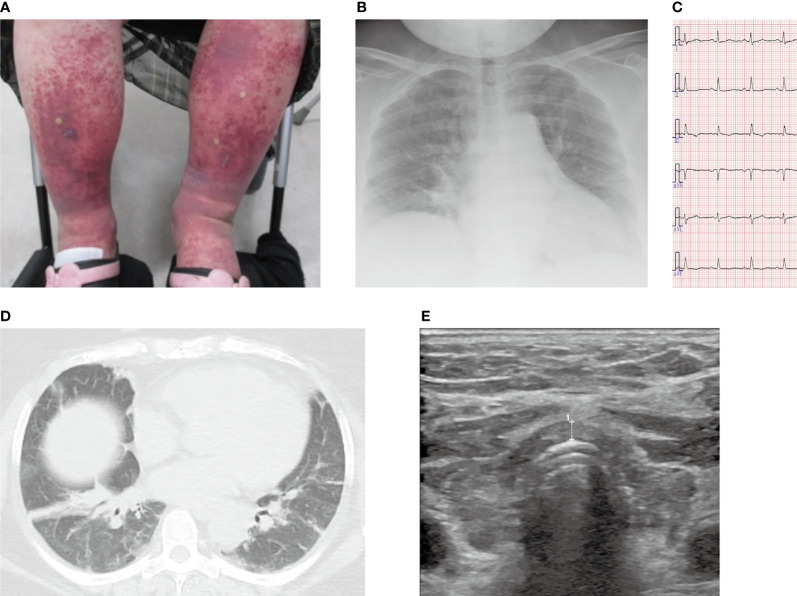
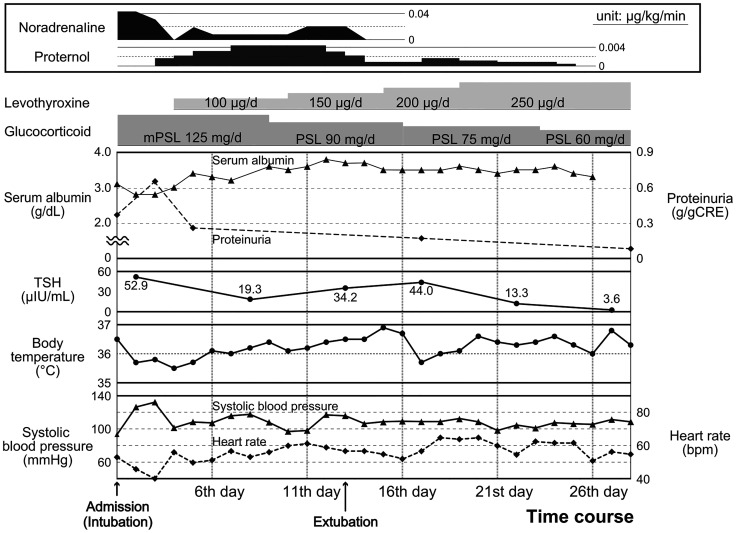
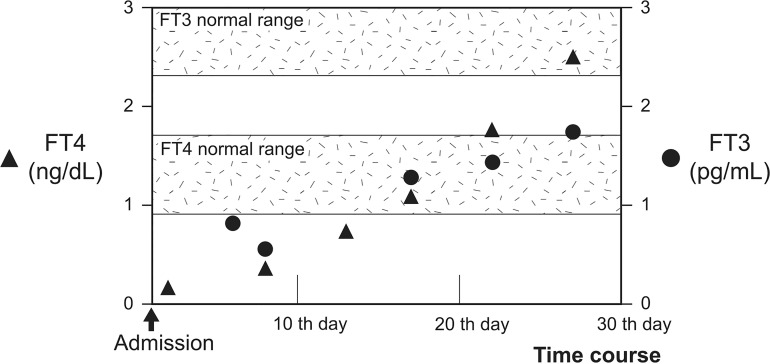
Myxedema coma is a critical disorder with high mortality rates. Disruption of the compensatory mechanism for severe and long-term hypothyroidism by various causes leads to critical conditions, including hypothermia, respiratory failure, circulatory failure, and central nervous system dysfunction. Infectious diseases, stroke, myocardial infarction, sedative drugs, and cold exposure are considered the main triggers for myxedema coma. A 59-year-old Japanese woman presented with bilateral painful purpura on her lower legs. She was diagnosed with coexisting immunoglobulin A (IgA) vasculitis and severe IgA vasculitis with nephritis and was consequently treated with intravenous methylprednisolone (125 mg/day). However, she rapidly developed multiple organ failure due to the exacerbation of severe hypothyroidism, i.e., myxedema. Her condition improved significantly following oral administration of prednisolone along with thyroxine. There was a delayed increase in the serum free triiodothyronine level, while the serum free thyroxine level was quickly restored to normal. Rapid deterioration of the patient's condition after admission led us to diagnose her as having myxedema coma triggered by IgA vasculitis. Hence, clinicians should be aware of the risks of dynamic exacerbations in patients with hypothyroidism. Furthermore, our study suggested that combination therapy with thyroxine and liothyronine might prove effective for patients with myxedema coma, especially for those who require high-dose glucocorticoid administration.
Keywords: Hashimoto’s thyroiditis; IgA vasculitis; glucocorticoid; levothyroxine; liothyronine; myxedema coma.
Copyright © 2022 Ito, Fukuda, Ashida, Nagayama, Sako, Mizuochi, Kabashima, Yoshinobu, Iwata, Hasuzawa, Hayashi, Akashi and Nomura.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
A case of fatal myxedema coma with electrocardiogram Osborne J-wave in a patient initially diagnosed with hypothyroidism.Endocr J. 2022 Sep 28;69(9):1109-1115. doi: 10.1507/endocrj.EJ21-0720. Epub 2022 Apr 9. Endocr J. 2022. PMID: 35400676
-
Successful treatment of myxedema coma with a combination of levothyroxine and liothyronine.Endocr J. 2019 May 28;66(5):469-474. doi: 10.1507/endocrj.EJ18-0469. Epub 2019 Mar 8. Endocr J. 2019. PMID: 30853666
-
Myxedema coma in a patient with subclinical hypothyroidism.Thyroid. 2011 Jan;21(1):87-9. doi: 10.1089/thy.2010.0175. Epub 2010 Nov 8. Thyroid. 2011. PMID: 21058937
-
Myxedema coma: diagnosis and treatment.Am Fam Physician. 2000 Dec 1;62(11):2485-90. Am Fam Physician. 2000. PMID: 11130234 Review.
-
[Myxedema coma].Medicina (B Aires). 2017;77(4):321-328. Medicina (B Aires). 2017. PMID: 28825577 Review. Spanish.
Cited by
-
Delayed Diagnosis of Myxedema Coma in a Patient With Concurrent Severe Intracranial Atherosclerotic Disease.Cureus. 2025 May 2;17(5):e83339. doi: 10.7759/cureus.83339. eCollection 2025 May. Cureus. 2025. PMID: 40452692 Free PMC article.
-
Type 3 autoimmune polyglandular syndrome (APS-3) or type 3 multiple autoimmune syndrome (MAS-3): an expanding galaxy.J Endocrinol Invest. 2023 Apr;46(4):643-665. doi: 10.1007/s40618-022-01994-1. Epub 2023 Jan 7. J Endocrinol Invest. 2023. PMID: 36609775 Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous