

Desmoid Tumors Arising on the Mesenteric Surgical Scar of Abdominal Sarcomas
- PMID: 35251801
- PMCID: PMC8887548
- DOI: 10.7759/cureus.21727
Desmoid Tumors Arising on the Mesenteric Surgical Scar of Abdominal Sarcomas
Abstract
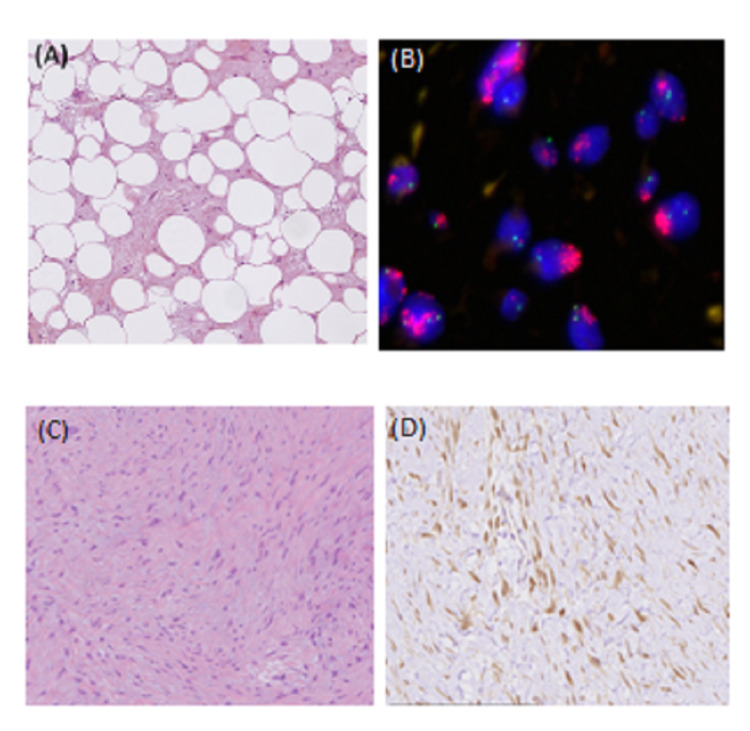
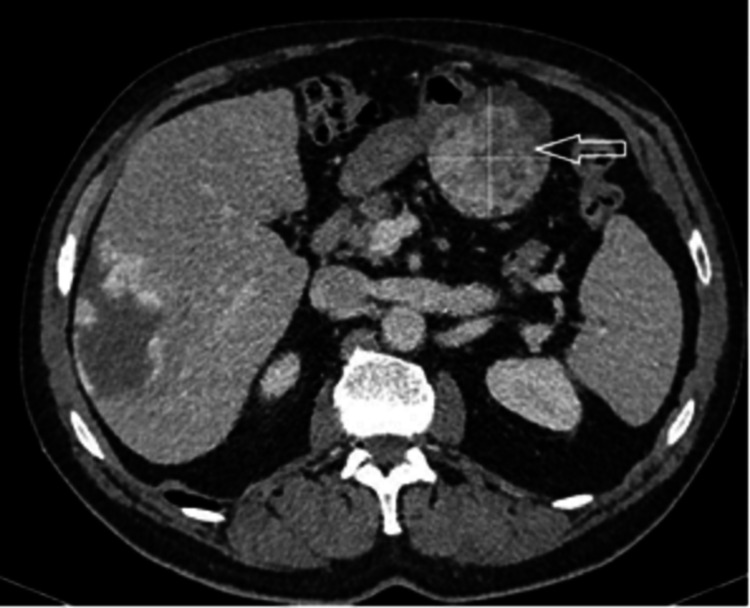
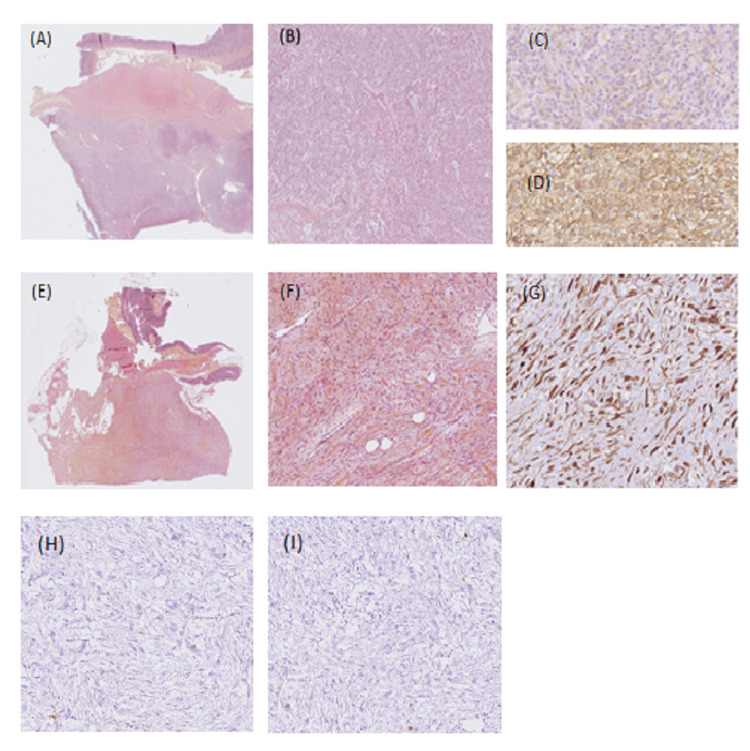
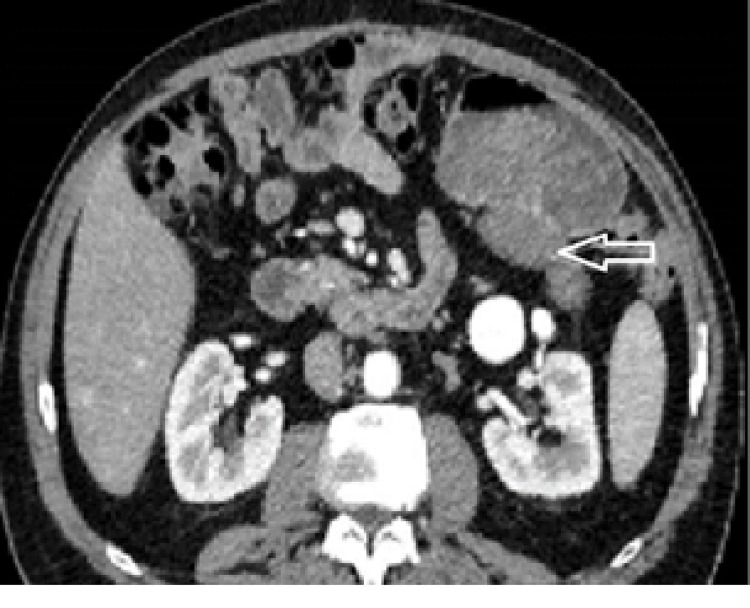
A sporadic desmoid tumor (DT) is a rare type of tumor of the mesenchymal connective tissues is now considered an intermediate disease or locally aggressive. They may develop on scars or after traumatism, favored by growth factors released during the initial phase of wound healing. Most of the abdominal DT arising on a scar is described on the wall incision. In this report, we describe two cases of DT arising on the intraperitoneal surgical scar, shortly after the resection of a low-grade retroperitoneal liposarcoma and a low-risk gastric gastrointestinal stromal tumor (GIST). Inconsistency between low risk according to the classification of the primary sarcoma and early local recurrence (LR) should raise the possibility of DT. Core needle biopsy (CNB) should be performed when it is feasible, including on local recurrences (LR). Surveillance has become the first-line treatment for DT. In case of progression between two imaging during the surveillance phase, surgery, when it's not mutilating, is indicated for selected cases as second-line treatment.
Keywords: desmoid tumor; mesenteric tumor; oncologic surgery; retroperitoneal tumor; sarcoma surgery; soft tissue tumor.
Copyright © 2022, Damiani et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


References
-
- World Health Organization. Lyon, France: IARC Press; [ Aug; 2021 ]. 2020. Soft Tissue and Bone Tumours. WHO Classification of Tumours, 5th Edition, Volume 3.
-
- The management of desmoid tumours: a joint global consensus-based guideline approach for adult and paediatric patients. Desmoid Tumor Working Group. Eur J Cancer. 2020;127:96–107. - PubMed
-
- Extra-abdominal primary fibromatosis: aggressive management could be avoided in a subgroup of patients. Bonvalot S, Eldweny H, Haddad V, et al. Eur J Surg Oncol. 2008;34:462–468. - PubMed
-
- Spontaneous regression of primary abdominal wall desmoid tumors: more common than previously thought. Bonvalot S, Ternès N, Fiore M, et al. Ann Surg Oncol. 2013;20:4096–4102. - PubMed
-
- Soft tissue and visceral sarcomas: ESMO-EURACAN-GENTURIS Clinical Practice Guidelines for diagnosis, treatment and follow-up. Gronchi A, Miah AB, Dei Tos AP, et al. Ann Oncol. 2021;32:1348–1365. - PubMed
Publication types
LinkOut - more resources
Full Text Sources