

Immunohistochemical Analysis of Postburn Scars following Treatment Using Dermal Substitutes
- PMID: 35251908
- PMCID: PMC8896958
- DOI: 10.1155/2022/3686863
Immunohistochemical Analysis of Postburn Scars following Treatment Using Dermal Substitutes
Abstract
Background: Post-burn hypertrophic scars commonly occur after burns. Studies that compare dermal substitutes with other treatment methods are insufficient. The purpose was to analyze the histopathological differences in hypertrophic burn scars after Matriderm®+split-thickness skin graft (STSG) and compare with AlloDerm®+STSG, STSG, full-thickness skin graft (FTSG), and normal skin.
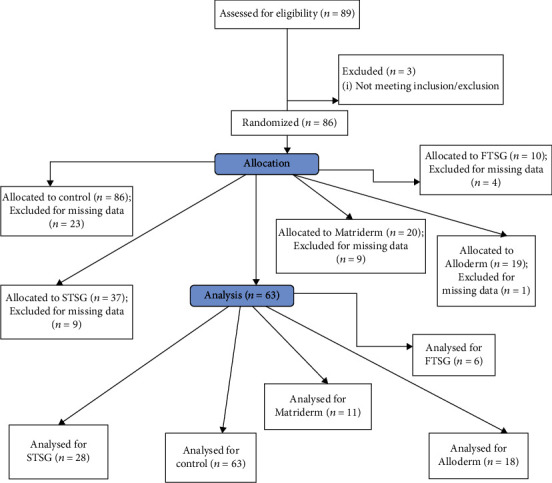
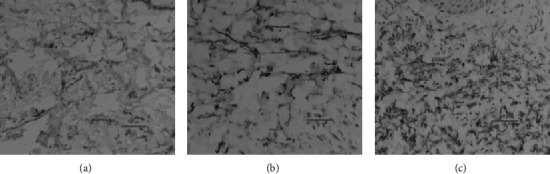
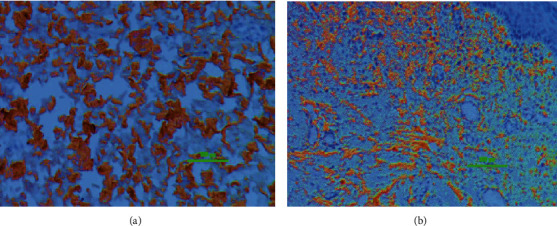
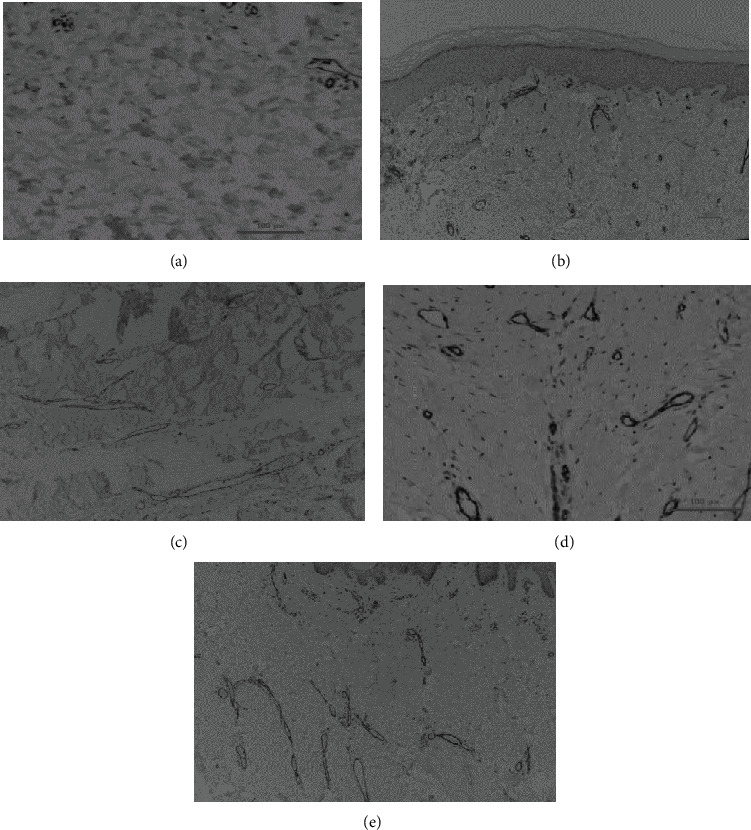
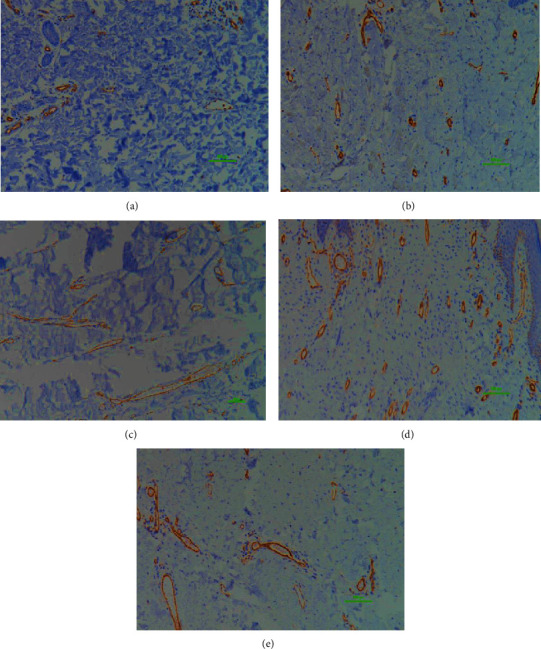
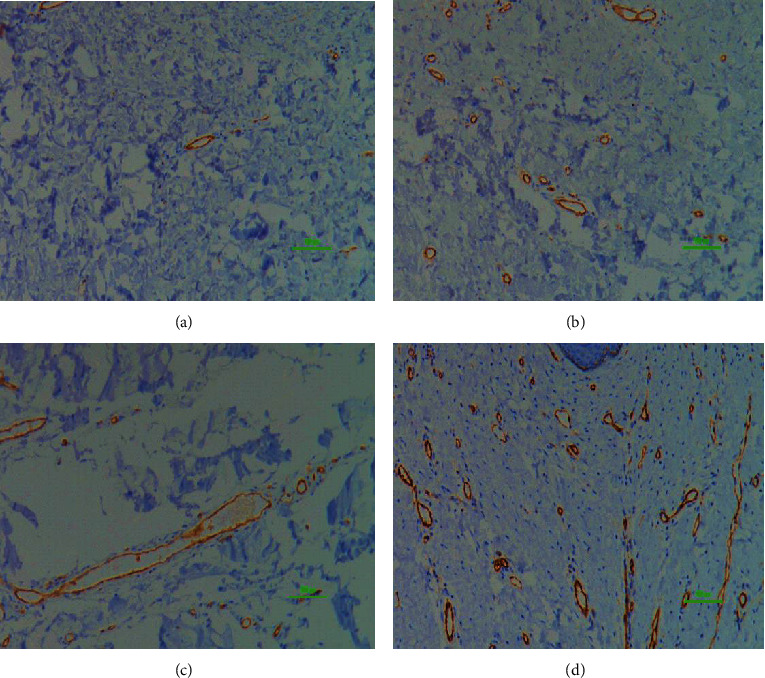
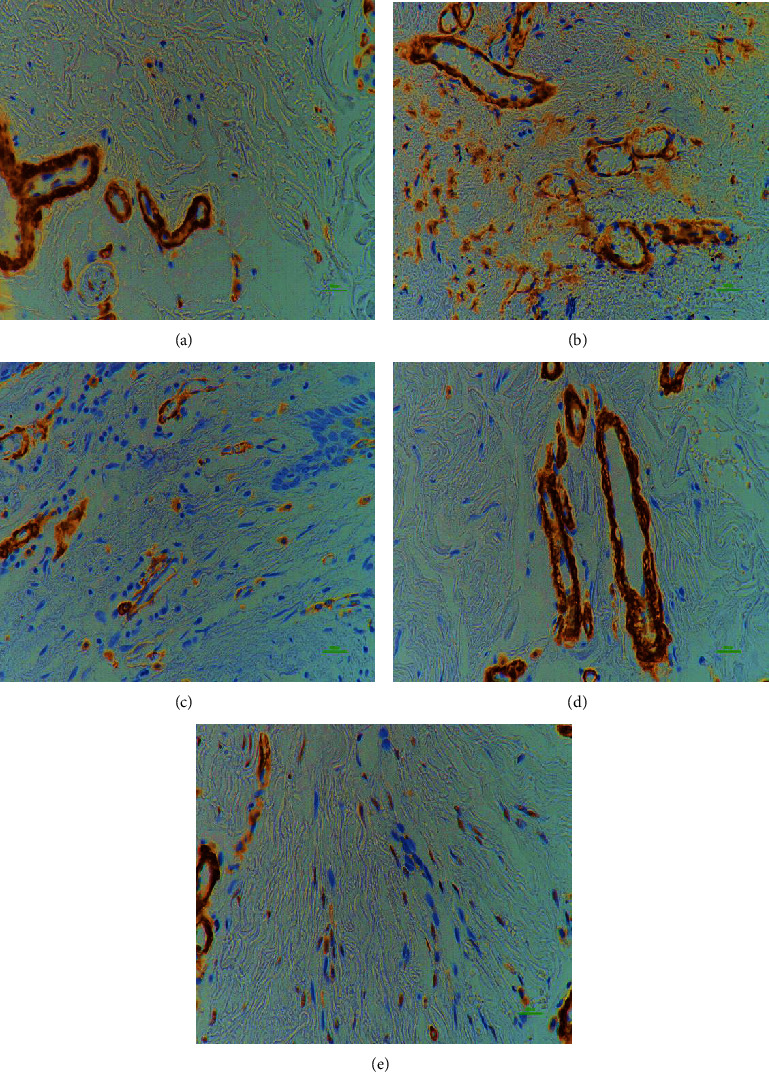
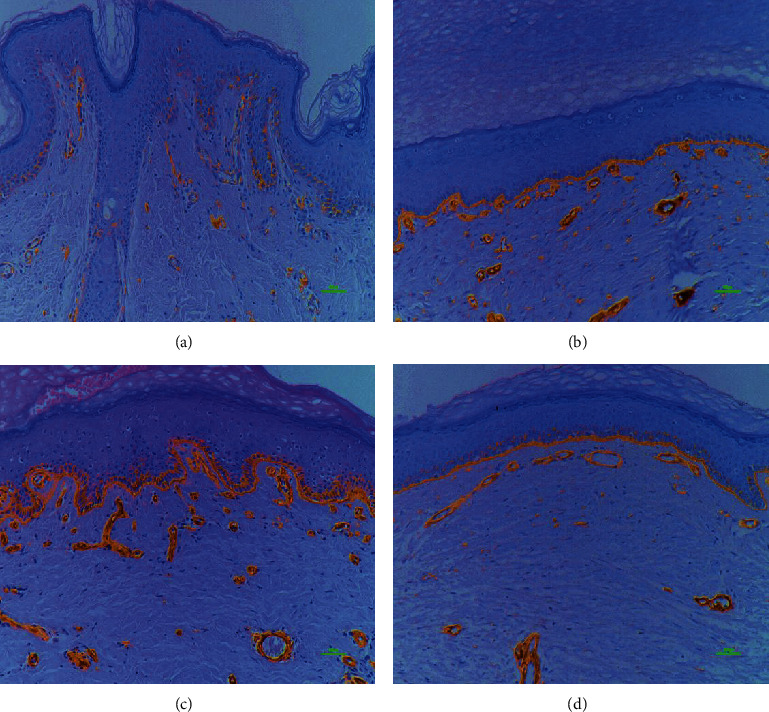
Methods: Samples of unburned, normal skin and deep 2nd or 3rd degree burns were obtained from patients who experienced a burn injury in the past to at least 6 months before biopsy, which was performed between 2011 and 2012. All subjects received >6 months of treatment before the biopsy. Intervention groups were normal (63), STSG (28), FTSG (6), Matriderm® (11), and AlloDerm® (18). Immunohistochemical analyses of elastin, collagen I, collagen III, cluster of differentiation 31 (CD31), smooth muscle actin (α-SMA), and laminin from scar and control tissues were performed and compared.
Results: α-SMA vascular quantity and vessel width, stromal CD31, and basement membrane laminin expression were not significantly different between normal and intervention groups. Matriderm® group showed no significant difference in elastin, collagen III, stromal CD31 and α-SMA, CD31 vessel width, stromal α-SMA, vessel quantity and width, and laminin length compared to the normal group, meaning they were not significantly different from the normal skin traits.
Conclusion: Dermal substitutes may be an optimal alternative to address the cosmetic and functional limitations posed by other treatment methods.
Copyright © 2022 Mi Young Lee et al.
Conflict of interest statement
None declared.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
