

Complete and Incomplete Resection for Progressive Glioblastoma Prolongs Post-Progression Survival
- PMID: 35251956
- PMCID: PMC8888692
- DOI: 10.3389/fonc.2022.755430
Complete and Incomplete Resection for Progressive Glioblastoma Prolongs Post-Progression Survival
Abstract
Objective: The role of resection in progressive glioblastoma (GBM) to prolong survival is still controversial. The aim of this study was to determine 1) the predictors of post-progression survival (PPS) in progressive GBM and 2) which subgroups of patients would benefit from recurrent resection.
Methods: We have conducted a retrospective bicentric cohort study on isocitrate dehydrogenase (IDH) wild-type GBM treated in our hospitals between 2006 and 2015. Kaplan-Maier analyses and univariable and multivariable Cox regressions were performed to identify predictors and their influence on PPS.
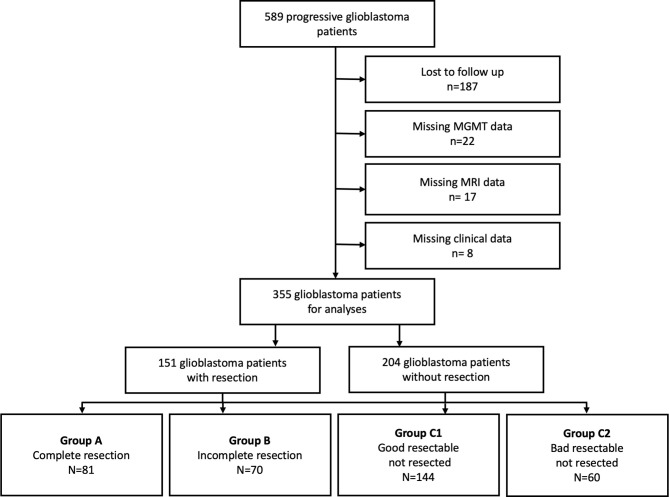
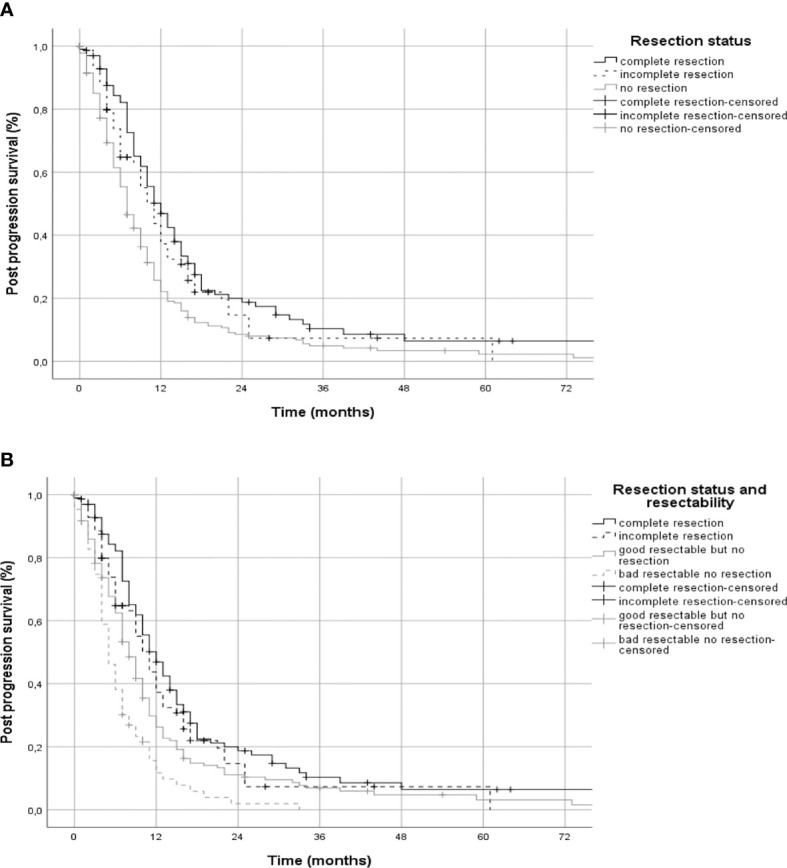
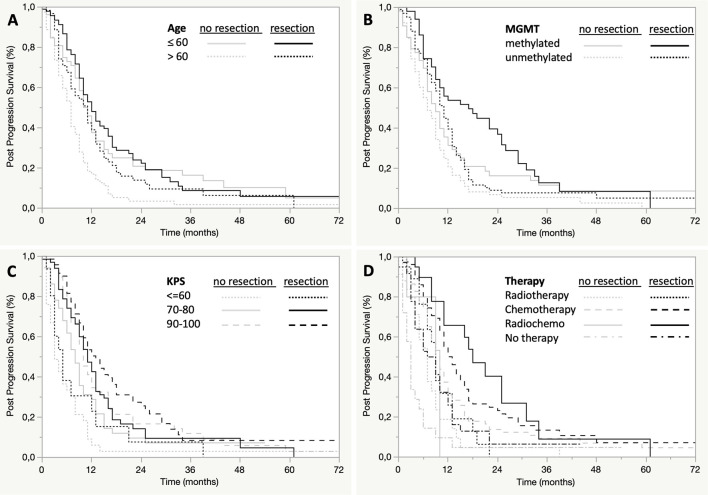
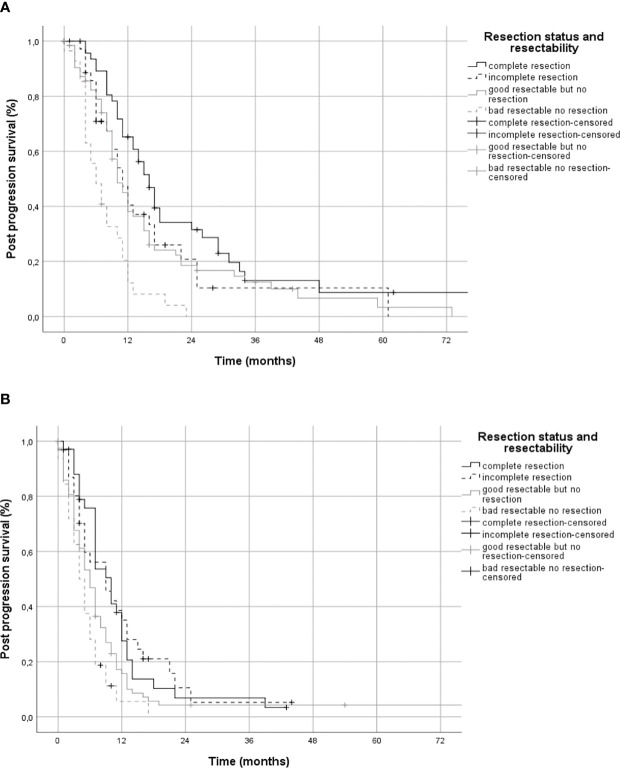
Results: Of 589 patients with progressive IDH wild-type GBM, 355 patients were included in analyses. Median PPS of all patients was 9 months (95% CI 8.0-10.0), with complete resection 12 months (95% CI 9.7-14.3, n=81), incomplete resection 11 months (95% CI 8.9-13.1, n=70) and without resection 7 months (95% CI 06-08, n=204). Multivariable Cox regression demonstrated a benefit for PPS with complete (HR 0.67, CI 0.49-0.90) and incomplete resection (HR 0.73, 95% CI 0.51-1.04) and confirmed methylation of the O6-methylguanine-DNA-methyltransferase (MGMT) gene promoter, lower age at diagnosis, absence of deep brain and multilocular localization, higher Karnofsky Performance Status (KPS) and recurrent therapies to be associated with longer PPS. In contrast, traditional eloquence and duration of progression-free survival had no effect on PPS. Subgroup analyses showed that all subgroups of confirmed predictors benefited from resection, except for patients in poor condition with a KPS <70.
Conclusions: Out data suggest a role for complete and incomplete recurrent resection in progressive GBM patients regardless of methylation of MGMT, age, or adjuvant therapy but not in patients with a poor clinical condition with a KPS <70.
Keywords: extent of resection; post progression survival; progressive glioblastoma; re-surgery; recurrent surgery; resectability; surgery.
Copyright © 2022 Behling, Rang, Dangel, Noell, Renovanz, Mäurer, Schittenhelm, Bender, Paulsen, Brendel, Martus, Gempt, Barz, Meyer, Tatagiba and Skardelly.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Wen PY, Weller M, Lee EQ, Alexander BM, Barnholtz-Sloan JS, Barthel FP, et al. . Glioblastoma in Adults: A Society for Neuro-Oncology (SNO) and European Society of Neuro-Oncology (EANO) Consensus Review on Current Management and Future Directions. Neuro-Oncology (2020) 22:1073–113. doi: 10.1093/neuonc/noaa106 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials