

Inferior Vena Cava Collapsibility Index Can Predict Hypotension and Guide Fluid Management After Spinal Anesthesia
- PMID: 35252337
- PMCID: PMC8891151
- DOI: 10.3389/fsurg.2022.831539
Inferior Vena Cava Collapsibility Index Can Predict Hypotension and Guide Fluid Management After Spinal Anesthesia
Abstract
Purpose: We hypothesized that inferior vena cava collapsibility index (IVCCI)-guided fluid management would reduce the incidence of postspinal anesthesia hypotension in patients undergoing non-cardiovascular, non-obstetric surgery.
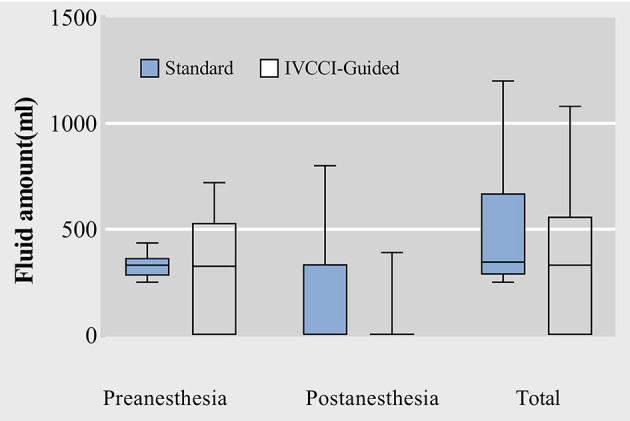
Methods: A receiver operating characteristic (ROC) curve was used to determine the diagnostic value of IVCCI for predicting hypotension after induction of spinal anesthesia and calculate the cut-off value. Based on the cut-off variation value, the following prospective randomized controlled trial aimed to compare the incidence of postspinal anesthesia hypotension between the IVCCI-guided fluid administration group and the standard fluid administration group. Secondary outcomes included the rate of vasoactive drug administration, the amount of fluid administered, and the incidence of nausea and vomiting.
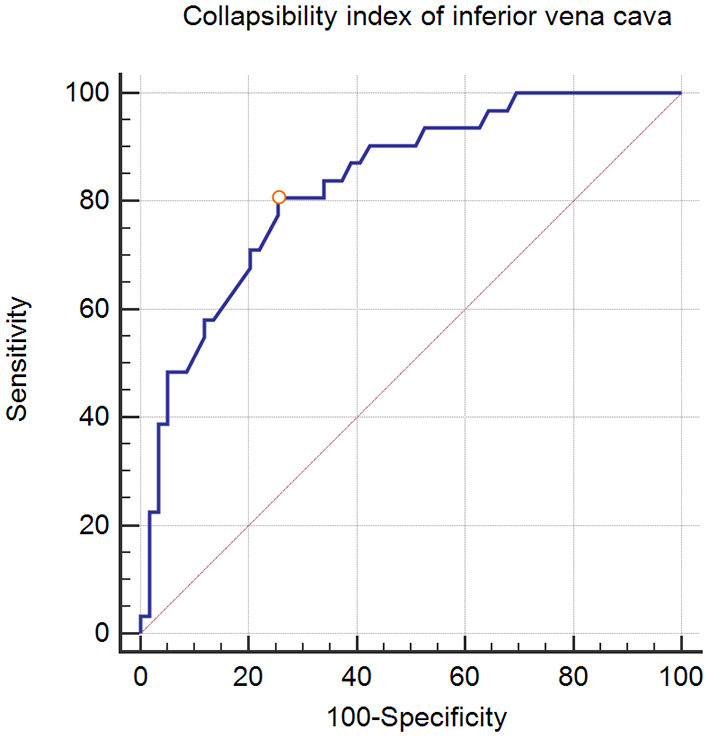
Results: ROC curve analysis revealed that IVCCI had a sensitivity of 83.9%, a specificity of 76.3%, and a positive predictive value of 84% for predicting postspinal anesthesia hypotension at a cut-off point of >42%. The area under the curve (AUC) was 0.834 (95% confidence interval: 0.740-0.904). According to the cut-off variation value of 42%, the IVCCI-guided group exhibited a lower incidence of hypotension than the standard group [9 (15.3%) vs. 20 (31.7%), P = 0.032]. Total fluid administered was lower in the IVCCI-guided group than in the standard group [330 (0-560) mL vs. 345 (285-670) mL, P = 0.030].
Conclusions: Prespinal ultrasound scanning of the IVCCI provides a reliable predictor of hypotension following spinal anesthesia at a cut-off point of >42%. IVCCI-guided fluid management before spinal anesthesia can reduce the incidence of hypotension following spinal anesthesia.
Keywords: hypotension; inferior vena cava collapsibility index; inferior vena cava ultrasound; intravascular volume; spinal anesthesia.
Copyright © 2022 Ni, Zhou, He and Zhou.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Assessing the Efficacy of Inferior Vena Cava Collapsibility Index for Predicting Hypotension after Central Neuraxial Block: A Systematic Review and Meta-Analysis.Diagnostics (Basel). 2023 Aug 31;13(17):2819. doi: 10.3390/diagnostics13172819. Diagnostics (Basel). 2023. PMID: 37685357 Free PMC article. Review.
-
Pre-operative ultrasonographic evaluation of inferior vena cava collapsibility index and caval aorta index as new predictors for hypotension after induction of spinal anaesthesia: A prospective observational study.Eur J Anaesthesiol. 2019 Apr;36(4):297-302. doi: 10.1097/EJA.0000000000000956. Eur J Anaesthesiol. 2019. PMID: 30664523
-
Inferior vena cava collapsibility index for predicting hypotension after spinal anesthesia in patients undergoing total knee arthroplasty.Anaesthesiologie. 2024 Nov;73(11):735-742. doi: 10.1007/s00101-024-01468-4. Epub 2024 Oct 9. Anaesthesiologie. 2024. PMID: 39382631 English.
-
Role of inferior vena cava collapsibility index in the prediction of hypotension associated with general anesthesia: an observational study.BMC Anesthesiol. 2019 Aug 7;19(1):139. doi: 10.1186/s12871-019-0809-4. BMC Anesthesiol. 2019. PMID: 31390983 Free PMC article.
-
Advances in the application of ultrasonographic parameters for fluid management in obstetric anesthesia.Am J Transl Res. 2024 Oct 15;16(10):5981-5989. doi: 10.62347/QMYL9341. eCollection 2024. Am J Transl Res. 2024. PMID: 39544761 Free PMC article. Review.
Cited by
-
Can Ultrasound-Guided Femoral Vein Measurements Predict Spinal Anesthesia-Induced Hypotension in Non-Obstetric Surgery? A Prospective Observational Study.Medicina (Kaunas). 2022 Nov 9;58(11):1615. doi: 10.3390/medicina58111615. Medicina (Kaunas). 2022. PMID: 36363572 Free PMC article.
-
The use of preoperative inferior vena cava ultrasound to predict anaesthesia-induced hypotension: a systematic review.Anaesthesiol Intensive Ther. 2023;55(1):18-31. doi: 10.5114/ait.2023.125310. Anaesthesiol Intensive Ther. 2023. PMID: 37306268 Free PMC article.
-
Passive Leg-Raising Test as a Predictor for the Drop in Blood Pressure After a Lumbar Epidural Block in the Pain Clinic: A Prospective Observational Study.J Clin Med. 2025 Apr 11;14(8):2629. doi: 10.3390/jcm14082629. J Clin Med. 2025. PMID: 40283461 Free PMC article.
-
Assessing the Efficacy of Inferior Vena Cava Collapsibility Index for Predicting Hypotension after Central Neuraxial Block: A Systematic Review and Meta-Analysis.Diagnostics (Basel). 2023 Aug 31;13(17):2819. doi: 10.3390/diagnostics13172819. Diagnostics (Basel). 2023. PMID: 37685357 Free PMC article. Review.
-
Efficacy of inferior vena cava collapsibility index and caval aorta index in predicting the incidence of hypotension after spinal anaesthesia- A prospective, blinded, observational study.Indian J Anaesth. 2023 Jun;67(6):523-529. doi: 10.4103/ija.ija_890_22. Epub 2023 Jun 14. Indian J Anaesth. 2023. PMID: 37476444 Free PMC article.
References
LinkOut - more resources
Full Text Sources