

The long-term effects of free care on birth outcomes: Evidence from a national policy reform in Zambia
- PMID: 35252533
- PMCID: PMC8889414
- DOI: 10.1016/j.ssmph.2022.101051
The long-term effects of free care on birth outcomes: Evidence from a national policy reform in Zambia
Abstract
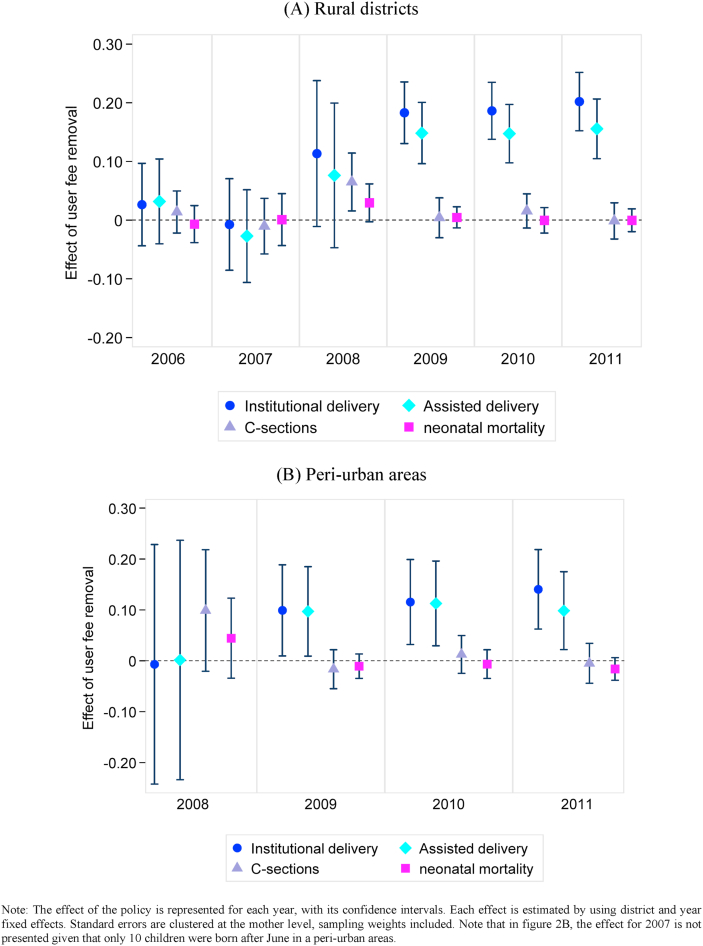
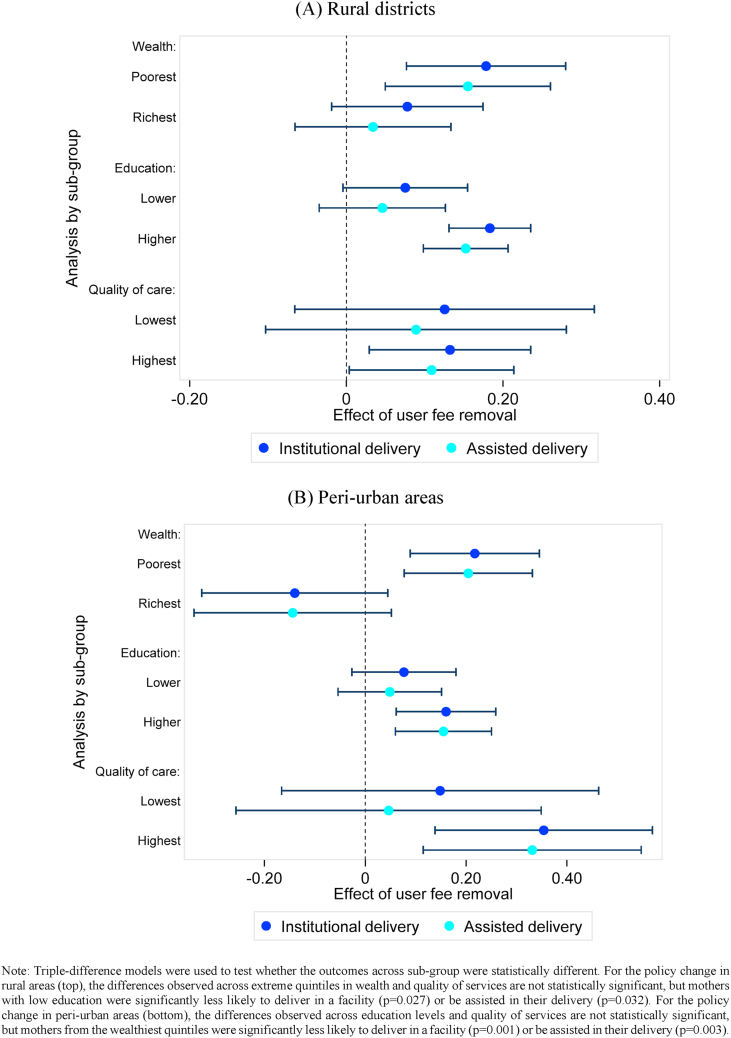
As women in many countries still fail to give birth in facilities due to financial barriers, many see the abolition of user fees as a key step on the path towards universal coverage. We exploited the staggered removal of user charges in Zambia from 2006 to estimate the effect of user fee removal up to five years after the policy change. We used data from the birth histories of two nationally representative Demographic and Health Surveys to implement a difference-in-differences analysis and identify the causal impact of removing user charges on institutional and assisted deliveries, caesarean sections and neonatal deaths. We also explored heterogeneous effects of the policy. Removing fees had little effect in the short term but large positive effects appeared about two years after the policy change. Institutional deliveries in treated areas increased by 10 and 15 percentage points in peri-urban and rural districts respectively (corresponding to a 25 and 35 percent change), driven entirely by a reduction in home births. However, there was no evidence that the reform changed the behaviours of women with lower education, the proportion of caesarean sections or reduced neonatal mortality. Institutional deliveries increased where care quality was high, but not where it was low. While abolishing user charges may reduce financial hardship from healthcare payments, it does not necessarily improve equitable access to care or health outcomes. Shifting away from user fees is a necessary but insufficient step towards universal health coverage, and concurrent reforms are needed to target vulnerable populations and improve quality of care.
Keywords: Care-seeking; Maternal care; Neonatal mortality; User fees; Zambia.
© 2022 Published by Elsevier Ltd.
Conflict of interest statement
Collins Chansa was working in the Ministry of Health of the Government of Zambia at the time of the health financing reform evaluated in this paper.
Figures
References
-
- Akin J.S., Griffin C.C., Guilkey D.K., Popkin B.M. The demand for primary health care services in the Bicol region of the Philippines. Economic Development and Cultural Change. 1986:755–782.
-
- Ansah E.K., Narh-Bana S., Asiamah S., Dzordzordzi V., Biantey K., Dickson K., Gyapong J.O., Koram K.A., Greenwood B.M., Mills A., Whitty C.J.M. Effect of removing direct payment for health care on utilisation and health outcomes in Ghanaian children: A randomised controlled trial. PLoS Medicine. 2009;6(1) - PMC - PubMed
-
- Ashraf N., Field E., Rusconi G., Voena A., Ziparo R. Traditional beliefs and learning about maternal risk in Zambia. The American Economic Review. 2017;107(5):511–515. - PubMed
-
- Bates I., Chapotera G., McKew S., Van Den Broek N. Maternal mortality in sub‐Saharan Africa: The contribution of ineffective blood transfusion services. BJOG: An International Journal of Obstetrics and Gynaecology. 2008;115(11):1331–1339. - PubMed
-
- Belizán J.M., Minckas N., McClure E.M., Saleem S., Moore J.L., Goudar S.S., Esamai F., Patel A., Chomba E., Garces A.L., Althabe F., Harrison M.S., Krebs N.F., Derman R.J., Carlo W.A., Liechty E.A., Hibberd P.L., Buekens P.M., Goldenberg R.L. An approach to identify a minimum and rational proportion of caesarean sections in resource-poor settings: A global network study. Lancet Global Health. 2018;6(8) e894–e901. - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
