

Mortality from drug-resistant tuberculosis in high-burden countries comparing routine drug susceptibility testing with whole-genome sequencing: a multicentre cohort study
- PMID: 35252901
- PMCID: PMC8896764
- DOI: 10.1016/S2666-5247(21)00044-6
Mortality from drug-resistant tuberculosis in high-burden countries comparing routine drug susceptibility testing with whole-genome sequencing: a multicentre cohort study
Abstract
Background: Drug resistance threatens global tuberculosis control. We aimed to examine mortality in patients with tuberculosis from high-burden countries, according to concordance or discordance of results from drug susceptibility testing done locally and whole-genome sequencing (WGS).
Methods: In this multicentre cohort study, we collected pulmonary Mycobacterium tuberculosis isolates and clinical data from individuals with tuberculosis from antiretroviral therapy programmes and tuberculosis clinics in Côte d'Ivoire, Democratic Republic of the Congo, Kenya, Nigeria, Peru, South Africa, and Thailand, stratified by HIV status and drug resistance. Sites tested drug susceptibility using routinely available methods. WGS was done on Illumina HiSeq 2500 in the USA and Switzerland, and TBprofiler was used to analyse the genomes. We included individuals aged 16 years or older with pulmonary tuberculosis (bacteriologically confirmed or clinically diagnosed). We analysed mortality in multivariable logistic regression models adjusted for sex, age, HIV status, history of tuberculosis, and sputum positivity.
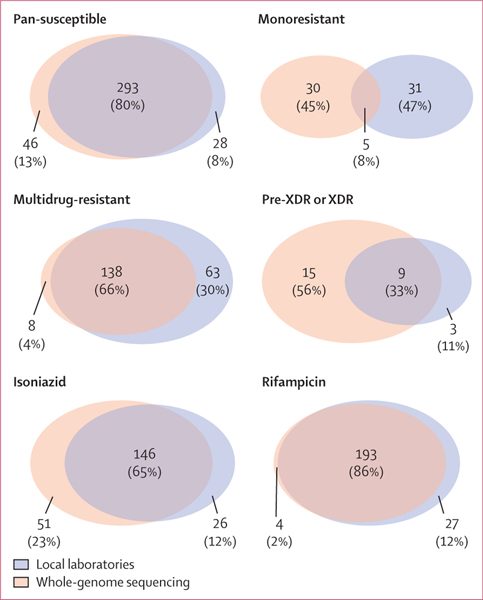
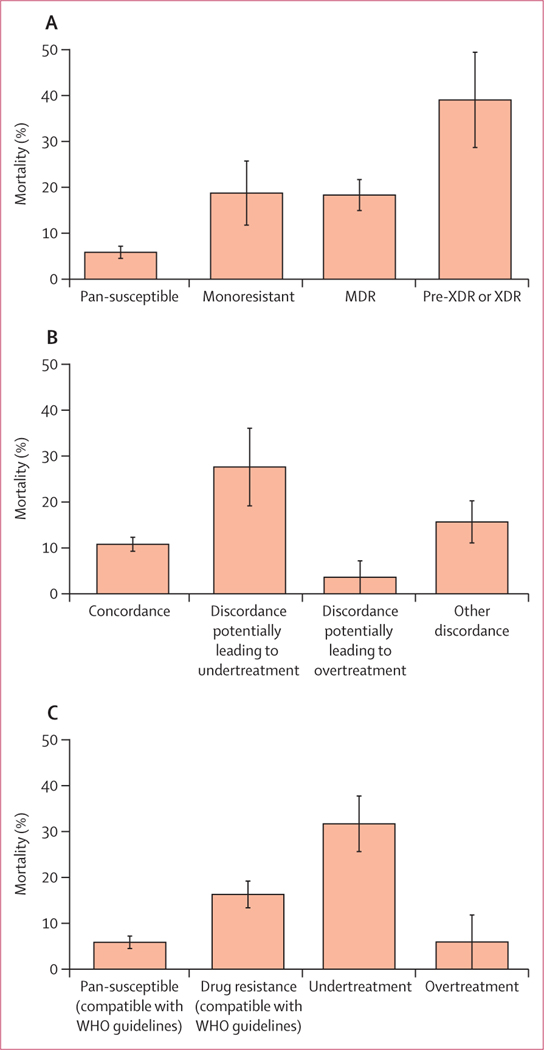
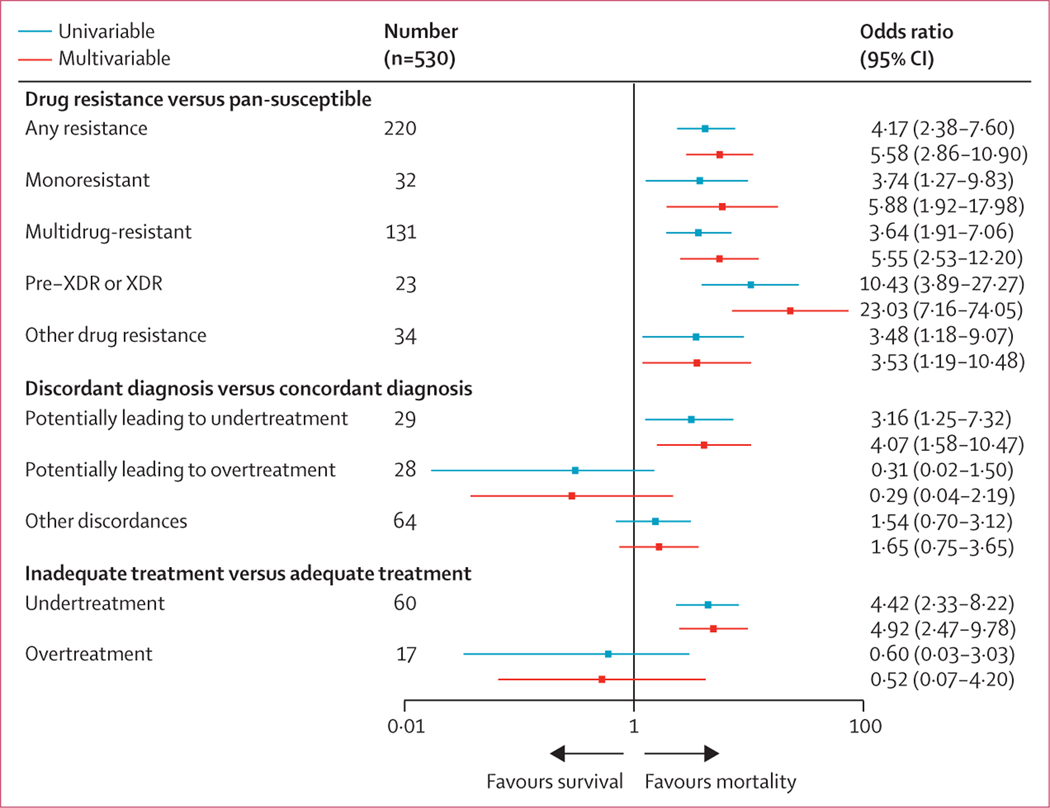
Findings: Between Sept 1, 2014, and July 4, 2016, of 634 patients included in our previous analysis, we included 582 patients with tuberculosis (median age 33 years [IQR 27-43], 225 [39%] women, and 247 [42%] HIV-positive). Based on WGS, 339 (58%) isolates were pan-susceptible, 35 (6%) monoresistant, 146 (25%) multidrug-resistant, and 24 (4%) pre-extensively drug-resistant (pre-XDR) or XDR. The analysis of mortality was based on 530 patients; 63 (12%) died and 77 (15%) patients received inappropriate treatment. Mortality ranged from 6% (18 of 310) in patients with pan-susceptible tuberculosis to 39% (nine of 23) in patients with pre-XDR or XDR tuberculosis. The adjusted odds ratio for mortality was 4·92 (95% CI 2·47-9·78) among undertreated patients, compared with appropriately treated patients.
Interpretation: In seven countries with a high burden of tuberculosis, we observed discrepancies between drug resistance patterns obtained locally and WGS. The underdiagnosis of drug resistance resulted in inappropriate treatment and higher mortality. WGS can provide accurate and detailed drug resistance information required to improve the outcomes of drug-resistant tuberculosis in high-burden settings. Our results support WHO's call for point-of-care tests based on WGS.
Funding: National Institutes of Allergy and Infectious Diseases, Swiss National Science Foundation, and Swiss National Center for Mycobacteria.
Figures
References
-
- WHO. Global tuberculosis report 2020. Geneva: World Health Organization, 2020. https://www.who.int/publications/i/item/9789240013131 (accessed April 28, 2020).
-
- Gandhi NR, Nunn P, Dheda K, et al. Multidrug-resistant and extensively drug-resistant tuberculosis: a threat to global control of tuberculosis. Lancet 2010; 375: 1830–43. - PubMed
-
- Müller AM, Osório CS, Silva DR, Sbruzzi G, de Tarso P, Dalcin R. Interventions to improve adherence to tuberculosis treatment: systematic review and meta-analysis. Int J Tuberc Lung Dis 2018; 22: 731–40. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- 203135/WT_/Wellcome Trust/United Kingdom
- 104803/WT_/Wellcome Trust/United Kingdom
- U01 AI069923/AI/NIAID NIH HHS/United States
- U01 AI069911/AI/NIAID NIH HHS/United States
- U01 AI069907/AI/NIAID NIH HHS/United States
- WT_/Wellcome Trust/United Kingdom
- FC0010218/CRUK_/Cancer Research UK/United Kingdom
- U01 AI069924/AI/NIAID NIH HHS/United States
- U54 AG062334/AG/NIA NIH HHS/United States
- U01 AI096299/AI/NIAID NIH HHS/United States
- U01 AI069919/AI/NIAID NIH HHS/United States
- U01 AI069918/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous