

Risk of Mental Health Problems in Children and Youths Following Concussion
- PMID: 35254429
- PMCID: PMC8902648
- DOI: 10.1001/jamanetworkopen.2022.1235
Risk of Mental Health Problems in Children and Youths Following Concussion
Abstract
Importance: Concussion may exacerbate existing mental health issues. Little evidence exists on whether concussion is associated with the onset of new psychopathologies or long-term mental health problems.
Objective: To investigate associations between concussion and risk of subsequent mental health issues, psychiatric hospitalizations, self-harm, or suicides.
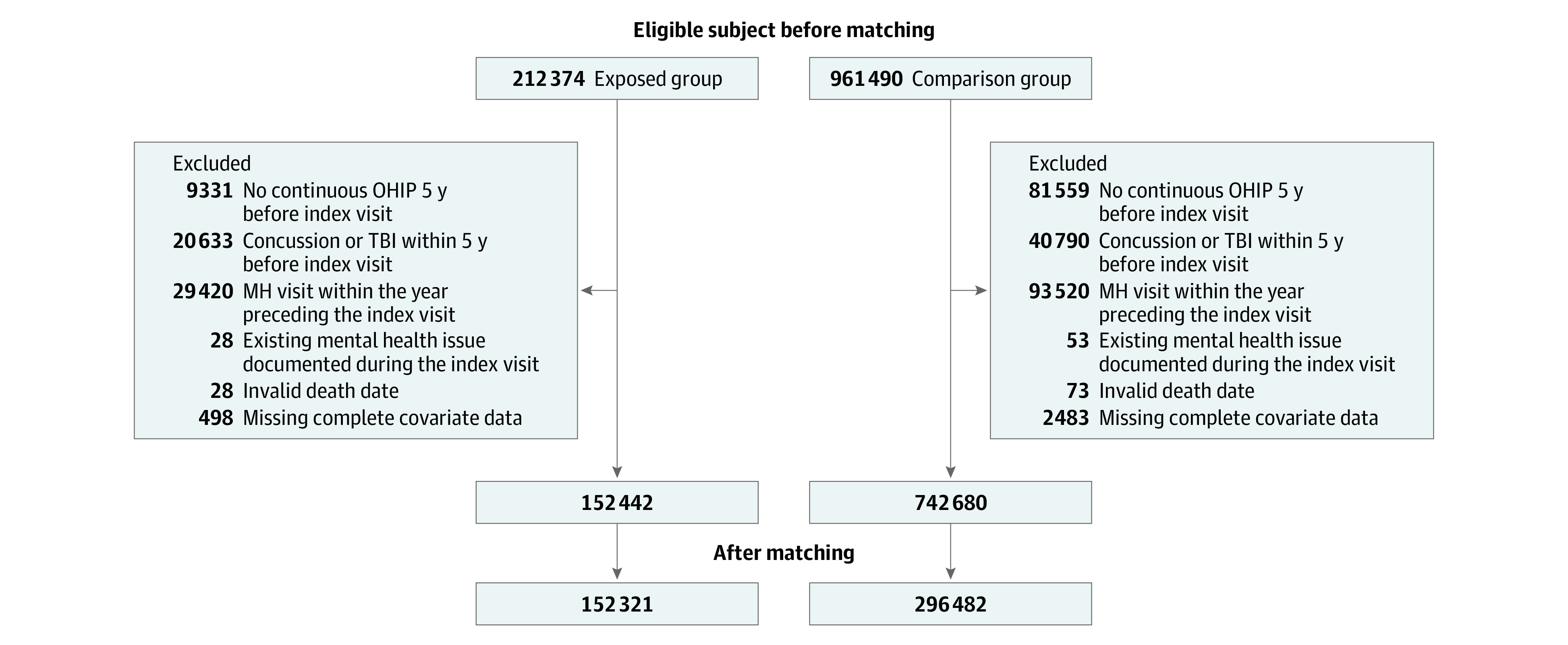
Design, setting, and participants: This population-based retrospective cohort study including children and youths aged 5 to 18 years with a concussion or orthopedic injury incurred between April 1, 2010, and March 31, 2020, in Ontario, Canada. Participants had no previous mental health visit in the year before the index event for cohort entry and no prior concussion or traumatic brain injury 5 years before the index visit. Data were collected from provincewide health administrative databases. Participants with concussion were included in the exposed cohort, and those with an orthopedic injury were included in the comparison cohort; these groups were matched 1:2, respectively, on age and sex.
Exposures: Concussion or orthopedic injury.
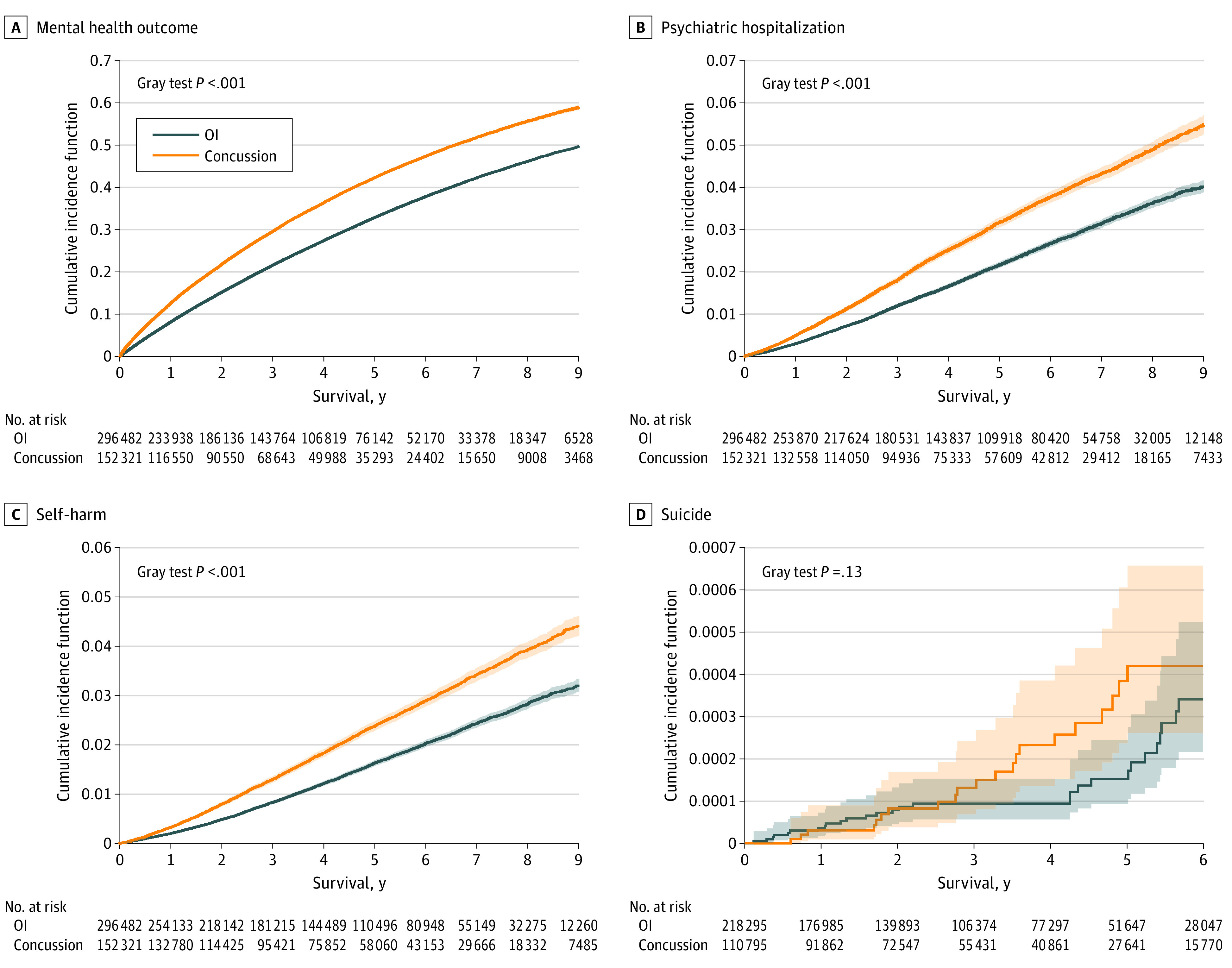
Main outcomes and measures: The primary outcome was mental health problems, such as psychopathologies and psychiatric disorders, identified from health care visits in emergency departments, hospitalizations, or primary care settings. Secondary outcomes were psychiatric hospitalizations, self-harm health care visits, and death by suicide (identified in health care or vital statistics databases).
Results: A total of 152 321 children and youths with concussion (median [IQR] age, 13 [10-16] years; 86 423 [56.7%] male) and 296 482 children and youths with orthopedic injury (median [IQR] age, 13 [10-16] years; 171 563 [57.9%] male) were matched by age and sex. The incidence rates of any mental health problem were 11 141 per 100 000 person-years (exposed group) and 7960 per 100 000 person-years (unexposed group); with a difference of 3181 (95% CI, 3073-3291) per 100 000 person-years. The exposed group had an increased risk of developing a mental health issue (adjusted hazard ratio [aHR], 1.39; 95% CI, 1.37-1.40), self-harm (aHR, 1.49; 95% CI, 1.42-1.56), and psychiatric hospitalization (aHR, 1.47; 95% CI, 1.41-1.53) after a concussion. There was no statistically significant difference in death by suicide between exposed and unexposed groups (HR, 1.54; 95% CI, 0.90-2.61).
Conclusions and relevance: Among children and youths aged 5 to 18 years, concussion was associated with an increased risk of mental health issues, psychiatric hospitalization, and self-harm compared with children and youths with an orthopedic injury.
Conflict of interest statement
Figures
Comment in
-
Contextual Considerations for the Increased Risk of Mental Health Problems Following Concussion in Youth.JAMA Netw Open. 2022 Mar 1;5(3):e221242. doi: 10.1001/jamanetworkopen.2022.1242. JAMA Netw Open. 2022. PMID: 35254435 No abstract available.
Similar articles
-
Premature Death, Suicide, and Nonlethal Intentional Self-Harm After Psychiatric Discharge.JAMA Netw Open. 2024 Jun 3;7(6):e2417131. doi: 10.1001/jamanetworkopen.2024.17131. JAMA Netw Open. 2024. PMID: 38922620 Free PMC article.
-
Association of Cannabis Use With Self-harm and Mortality Risk Among Youths With Mood Disorders.JAMA Pediatr. 2021 Apr 1;175(4):377-384. doi: 10.1001/jamapediatrics.2020.5494. JAMA Pediatr. 2021. PMID: 33464286 Free PMC article.
-
Self-Harm Events and Suicide Deaths Among Autistic Individuals in Ontario, Canada.JAMA Netw Open. 2023 Aug 1;6(8):e2327415. doi: 10.1001/jamanetworkopen.2023.27415. JAMA Netw Open. 2023. PMID: 37552480 Free PMC article.
-
Mental Health Hospitalizations in Canadian Children, Adolescents, and Young Adults Over the COVID-19 Pandemic.JAMA Netw Open. 2024 Jul 1;7(7):e2422833. doi: 10.1001/jamanetworkopen.2024.22833. JAMA Netw Open. 2024. PMID: 38976264 Free PMC article.
-
Association of Extracorporeal Membrane Oxygenation With New Mental Health Diagnoses in Adult Survivors of Critical Illness.JAMA. 2022 Nov 8;328(18):1827-1836. doi: 10.1001/jama.2022.17714. JAMA. 2022. PMID: 36286084 Free PMC article.
Cited by
-
Association between days for concussion recovery and initial specialty clinic evaluation within 48 hours.BMC Sports Sci Med Rehabil. 2024 Apr 2;16(1):75. doi: 10.1186/s13102-024-00866-w. BMC Sports Sci Med Rehabil. 2024. PMID: 38566116 Free PMC article.
-
Concussion history associated with adolescent psychological distress but not hazardous gambling: a cross-sectional study.BMC Psychol. 2024 Jun 5;12(1):329. doi: 10.1186/s40359-024-01830-6. BMC Psychol. 2024. PMID: 38840182 Free PMC article.
-
Pediatric Concussion Injuries in Soccer: Emergency Department Trends in the United States From 2012 to 2023.Orthop J Sports Med. 2024 Dec 3;12(12):23259671241303180. doi: 10.1177/23259671241303180. eCollection 2024 Dec. Orthop J Sports Med. 2024. PMID: 39628763 Free PMC article.
-
Mild Traumatic Brain Injuries and Risk for Affective and Behavioral Disorders.Pediatrics. 2024 Jan 1;153(2):e2023062340. doi: 10.1542/peds.2023-062340. Pediatrics. 2024. PMID: 38268428 Free PMC article.
-
Postconcussion Moderate to Vigorous Physical Activity Predicts Anxiety Severity among Adolescent Athletes.Med Sci Sports Exerc. 2024 May 1;56(5):790-795. doi: 10.1249/MSS.0000000000003368. Epub 2023 Dec 27. Med Sci Sports Exerc. 2024. PMID: 38181208 Free PMC article.
References
-
- Cassidy JD, Carroll LJ, Peloso PM, et al. ; WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury . Incidence, risk factors and prevention of mild traumatic brain injury: results of the WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. J Rehabil Med. 2004;(43)(suppl):28-60. doi:10.1080/16501960410023732 - DOI - PubMed
-
- US Centers for Disease Control and Prevention . Report to Congress: the management of traumatic brain injury in children. Accessed January 31, 2022. https://www.cdc.gov/traumaticbraininjury/pdf/reportstocongress/managemen...
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
