

Current controversies in TNM for the radiological staging of rectal cancer and how to deal with them: results of a global online survey and multidisciplinary expert consensus
- PMID: 35254485
- PMCID: PMC9213337
- DOI: 10.1007/s00330-022-08591-z
Current controversies in TNM for the radiological staging of rectal cancer and how to deal with them: results of a global online survey and multidisciplinary expert consensus
Abstract
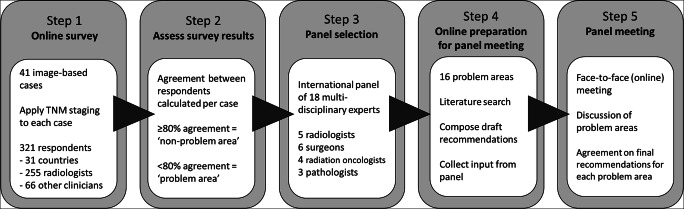
Objectives: To identify the main problem areas in the applicability of the current TNM staging system (8th ed.) for the radiological staging and reporting of rectal cancer and provide practice recommendations on how to handle them.
Methods: A global case-based online survey was conducted including 41 image-based rectal cancer cases focusing on various items included in the TNM system. Cases reaching < 80% agreement among survey respondents were identified as problem areas and discussed among an international expert panel, including 5 radiologists, 6 colorectal surgeons, 4 radiation oncologists, and 3 pathologists.
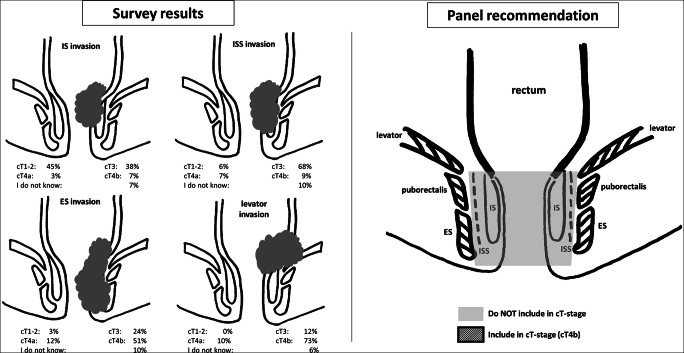
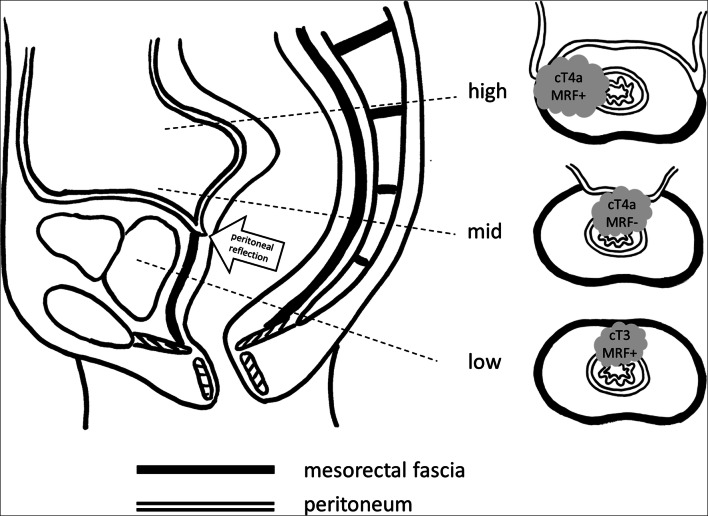
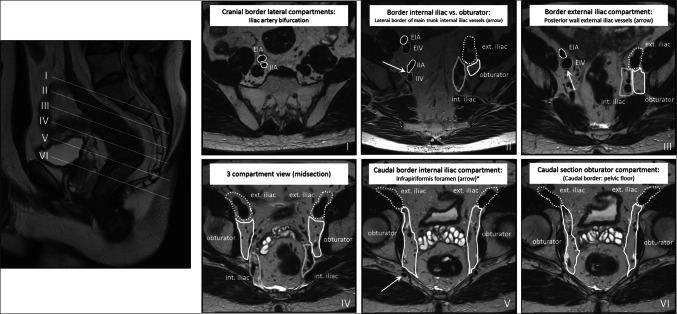
Results: Three hundred twenty-one respondents (from 32 countries) completed the survey. Sixteen problem areas were identified, related to cT staging in low-rectal cancers, definitions for cT4b and cM1a disease, definitions for mesorectal fascia (MRF) involvement, evaluation of lymph nodes versus tumor deposits, and staging of lateral lymph nodes. The expert panel recommended strategies on how to handle these, including advice on cT-stage categorization in case of involvement of different layers of the anal canal, specifications on which structures to include in the definition of cT4b disease, how to define MRF involvement by the primary tumor and other tumor-bearing structures, how to differentiate and report lymph nodes and tumor deposits on MRI, and how to anatomically localize and stage lateral lymph nodes.
Conclusions: The recommendations derived from this global survey and expert panel discussion may serve as a practice guide and support tool for radiologists (and other clinicians) involved in the staging of rectal cancer and may contribute to improved consistency in radiological staging and reporting.
Key points: • Via a case-based online survey (incl. 321 respondents from 32 countries), we identified 16 problem areas related to the applicability of the TNM staging system for the radiological staging and reporting of rectal cancer. • A multidisciplinary panel of experts recommended strategies on how to handle these problem areas, including advice on cT-stage categorization in case of involvement of different layers of the anal canal, specifications on which structures to include in the definition of cT4b disease, how to define mesorectal fascia involvement by the primary tumor and other tumor-bearing structures, how to differentiate and report lymph nodes and tumor deposits on MRI, and how to anatomically localize and stage lateral lymph nodes. • These recommendations may serve as a practice guide and support tool for radiologists (and other clinicians) involved in the staging of rectal cancer and may contribute to improved consistency in radiological staging and reporting.
Keywords: Consensus; Guideline; Magnetic resonance imaging; Neoplasm staging; Rectal neoplasms.
© 2022. The Author(s).
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Figures
References
-
- Jessup MJ, Goldberg RM, Asare EA, et al (2017) Colon and rectum. In: Amin MB, Edge S, Greene F, Byrd DR, Brookland RK, Washington MK, et al Eds. AJCC cancer staging manual (8th edition). Springer: 251–273
-
- Wittekind C, Greene FL, Henson DE, et al (2003) Explanatory notes specific anatomical sites. In: Wittekind Ch, Greene F.L, Henson D.E et al eds. TNM supplement: a commentary on uniform use 3rd edition. New York, NY. Wiley-Liss: 40–86
-
- Wittekind C, Brierly JD, Lee AWM, et al (2019) Explanatory notes specific anatomical sites. In: Wittekind C, Brierly J.D, Lee A.W.M, et al eds. TNM supplement: a commentary on uniform use. 5th edition. New York, NY. Wiley-Liss: 54–85
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
