

Physician Practices With Robust Capabilities Spend Less On Medicare Beneficiaries Than More Limited Practices
- PMID: 35254927
- PMCID: PMC8903048
- DOI: 10.1377/hlthaff.2021.00302
Physician Practices With Robust Capabilities Spend Less On Medicare Beneficiaries Than More Limited Practices
Abstract
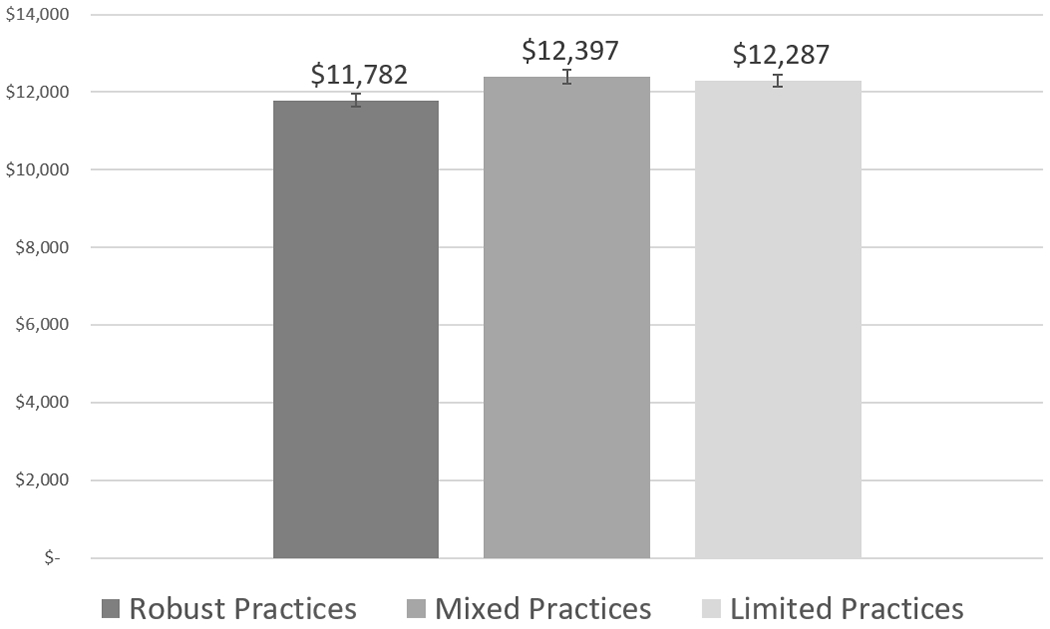
No research has considered a range of physician practice capabilities for managing patient care when examining practice-level influences on quality of care, utilization, and spending. Using data from the 2017 National Survey of Healthcare Organizations and Systems linked to 2017 Medicare fee-for-service claims data from attributed beneficiaries, we examined the association of practice-level capabilities with process measures of quality, utilization, and spending. In propensity score-weighted mixed-effects regression analyses, physician practice locations with "robust" capabilities had lower total spending compared to locations with "mixed" or "limited" capabilities. Quality and utilization, however, did not differ by practice-level capabilities. Physician practice locations with robust capabilities spend less on Medicare fee-for-service beneficiaries but deliver quality of care that is comparable to the quality delivered in locations with low or mixed capabilities. Reforms beyond those targeting practice capabilities, including multipayer alignment and payment reform, may be needed to support larger performance advantages for practices with robust capabilities.
Figures
Similar articles
-
Organizational integration, practice capabilities, and outcomes in clinically complex medicare beneficiaries.Health Serv Res. 2020 Dec;55 Suppl 3(Suppl 3):1085-1097. doi: 10.1111/1475-6773.13580. Epub 2020 Oct 26. Health Serv Res. 2020. PMID: 33104254 Free PMC article.
-
Changes in health care spending and quality for Medicare beneficiaries associated with a commercial ACO contract.JAMA. 2013 Aug 28;310(8):829-36. doi: 10.1001/jama.2013.276302. JAMA. 2013. PMID: 23982369 Free PMC article.
-
Physician- versus practice-level primary care continuity and association with outcomes in Medicare beneficiaries.Health Serv Res. 2022 Aug;57(4):914-929. doi: 10.1111/1475-6773.13999. Epub 2022 May 30. Health Serv Res. 2022. PMID: 35522231 Free PMC article.
-
Physician payment 2008 for interventionalists: current state of health care policy.Pain Physician. 2007 Sep;10(5):607-26. Pain Physician. 2007. PMID: 17876359 Review.
-
Issues in health care: interventional pain management at the crossroads.Pain Physician. 2007 Mar;10(2):261-84. Pain Physician. 2007. PMID: 17387349 Review.
Cited by
-
Changes in US Primary Care Access and Capabilities During the COVID-19 Pandemic.JAMA Health Forum. 2025 Feb 7;6(2):e245237. doi: 10.1001/jamahealthforum.2024.5237. JAMA Health Forum. 2025. PMID: 39918830 Free PMC article.
-
Improving health equity through health care systems research.Health Serv Res. 2023 Dec;58 Suppl 3(Suppl 3):289-299. doi: 10.1111/1475-6773.14192. Health Serv Res. 2023. PMID: 38015859 Free PMC article.
References
-
- Shrank WH, Rogstad TL, Parekh N. Waste in the US health care system: estimated costs and potential for savings. JAMA. 2019;322(15):1501–9. - PubMed
-
- Liao JM, Navathe AS, Werner RM. The impact of Medicare’s alternative payment models on the value of care. Annu Rev Public Health. 2020;41:551–65. - PubMed
-
- Peikes D, Dale S, Ghosh A, Taylor EF, Swankoski K, O’Malley AS, et al. The Comprehensive Primary Care Initiative: effects on spending, quality, patients, and physicians. Health Aff (Millwood). 2018;37(6):890–9. - PubMed
-
- Weeks WB, Gottlieb DJ, Nyweide DE, Sutherland JM, Bynum J, Casalino LP, et al. Higher health care quality and bigger savings found at large multispecialty medical groups. Health Aff (Millwood). 2010;29(5):991–7. - PubMed