

Pan-ebolavirus serology study of healthcare workers in the Mbandaka Health Region, Democratic Republic of the Congo
- PMID: 35255093
- PMCID: PMC8929691
- DOI: 10.1371/journal.pntd.0010167
Pan-ebolavirus serology study of healthcare workers in the Mbandaka Health Region, Democratic Republic of the Congo
Abstract
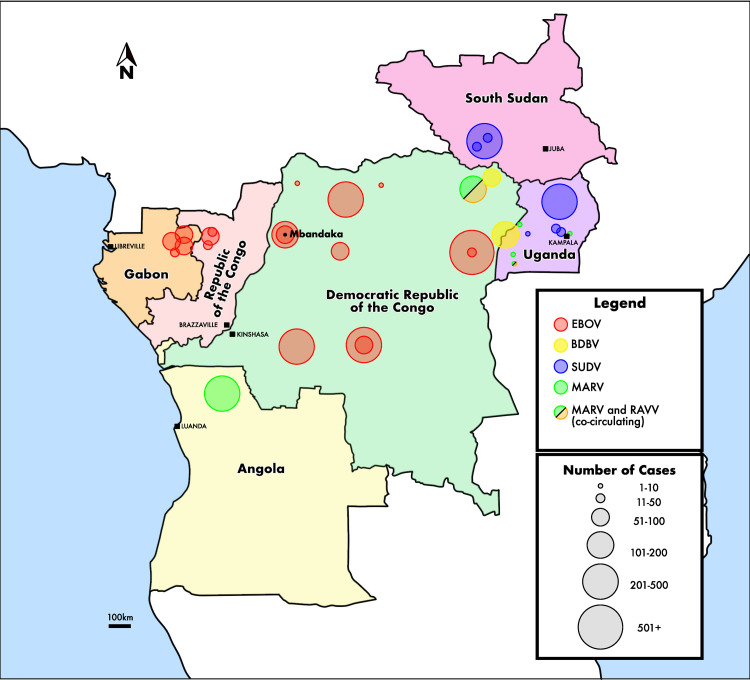
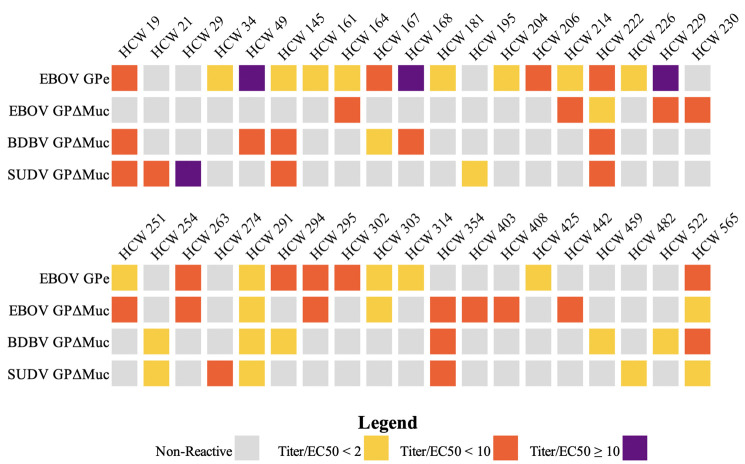
Although multiple antigenically distinct ebolavirus species can cause human disease, previous serosurveys focused on only Zaire ebolavirus (EBOV). Thus, the extent of reactivity or exposure to other ebolaviruses, and which sociodemographic factors are linked to this seroreactivity, are unclear. We conducted a serosurvey of 539 healthcare workers (HCW) in Mbandaka, Democratic Republic of the Congo, using ELISA-based analysis of serum IgG against EBOV, Sudan ebolavirus (SUDV) and Bundibugyo ebolavirus (BDBV) glycoproteins (GP). We compared seroreactivity to risk factors for viral exposure using univariate and multivariable logistic regression. Seroreactivity against different GPs ranged from 2.2-4.6%. Samples from six individuals reacted to all three species of ebolavirus and 27 samples showed a species-specific IgG response. We find that community health volunteers are more likely to be seroreactive against each antigen than nurses, and in general, that HCWs with indirect patient contact have higher anti-EBOV GP IgG levels than those with direct contact. Seroreactivity against ebolavirus GP may be associated with positions that offer less occupational training and access to PPE. Those individuals with broadly reactive responses may have had multiple ebolavirus exposures or developed cross-reactive antibodies. In contrast, those individuals with species-specific BDBV or SUDV GP seroreactivity may have been exposed to an ebolavirus not previously known to circulate in the region.
Conflict of interest statement
The authors have declared that no competing interests exist. Author Nathalie Kavira was unable to confirm her authorship contributions. On her behalf, the corresponding author has reported her contributions to the best of their knowledge.
Figures
Similar articles
-
Pan-Filovirus Serum Neutralizing Antibodies in a Subset of Congolese Ebolavirus Infection Survivors.J Infect Dis. 2018 Nov 5;218(12):1929-1936. doi: 10.1093/infdis/jiy453. J Infect Dis. 2018. PMID: 30107445 Free PMC article.
-
Risk Factors for Ebola Exposure in Health Care Workers in Boende, Tshuapa Province, Democratic Republic of the Congo.J Infect Dis. 2022 Sep 4;226(4):608-615. doi: 10.1093/infdis/jiaa747. J Infect Dis. 2022. PMID: 33269402 Free PMC article.
-
Distinct Immunogenicity and Efficacy of Poxvirus-Based Vaccine Candidates against Ebola Virus Expressing GP and VP40 Proteins.J Virol. 2018 May 14;92(11):e00363-18. doi: 10.1128/JVI.00363-18. Print 2018 Jun 1. J Virol. 2018. PMID: 29514907 Free PMC article.
-
Zoonotic risk factors associated with seroprevalence of Ebola virus GP antibodies in the absence of diagnosed Ebola virus disease in the Democratic Republic of Congo.PLoS Negl Trop Dis. 2021 Aug 12;15(8):e0009566. doi: 10.1371/journal.pntd.0009566. eCollection 2021 Aug. PLoS Negl Trop Dis. 2021. PMID: 34383755 Free PMC article.
-
Achieving cross-reactivity with pan-ebolavirus antibodies.Curr Opin Virol. 2019 Feb;34:140-148. doi: 10.1016/j.coviro.2019.01.003. Epub 2019 Mar 15. Curr Opin Virol. 2019. PMID: 30884329 Free PMC article. Review.
Cited by
-
Low seroprevalence of Ebola virus in health care providers in an endemic region (Tshuapa province) of the Democratic Republic of the Congo.PLoS One. 2023 Sep 1;18(9):e0286479. doi: 10.1371/journal.pone.0286479. eCollection 2023. PLoS One. 2023. PMID: 37656725 Free PMC article.
-
Molecular adaptations during viral epidemics.EMBO Rep. 2022 Aug 3;23(8):e55393. doi: 10.15252/embr.202255393. Epub 2022 Jul 18. EMBO Rep. 2022. PMID: 35848484 Free PMC article. Review.
-
Epitope-focused immunogen design based on the ebolavirus glycoprotein HR2-MPER region.PLoS Pathog. 2022 May 18;18(5):e1010518. doi: 10.1371/journal.ppat.1010518. eCollection 2022 May. PLoS Pathog. 2022. PMID: 35584193 Free PMC article.
-
Seroprevalence of Antibodies to Filoviruses with Outbreak Potential in Sub-Saharan Africa: A Systematic Review to Inform Vaccine Development and Deployment.Vaccines (Basel). 2024 Dec 11;12(12):1394. doi: 10.3390/vaccines12121394. Vaccines (Basel). 2024. PMID: 39772055 Free PMC article. Review.
-
The rVSV-EBOV vaccine provides limited cross-protection against Sudan virus in guinea pigs.NPJ Vaccines. 2023 Jun 10;8(1):91. doi: 10.1038/s41541-023-00685-z. NPJ Vaccines. 2023. PMID: 37301890 Free PMC article.
References
-
- History of Ebola Virus Disease (EVD) outbreaks. 17 Jun 2021 [cited 7 Jul 2021]. Available: https://www.cdc.gov/vhf/ebola/history/chronology.html
-
- Qureshi AI. Clinical manifestations and laboratory diagnosis of Ebola virus infection. Ebola Virus Disease. Elsevier; 2016. pp. 117–138.
