

Association between maternal thyroid function and risk of gestational hypertension and pre-eclampsia: a systematic review and individual-participant data meta-analysis
- PMID: 35255260
- PMCID: PMC10314731
- DOI: 10.1016/S2213-8587(22)00007-9
Association between maternal thyroid function and risk of gestational hypertension and pre-eclampsia: a systematic review and individual-participant data meta-analysis
Abstract
Background: Adequate maternal thyroid function is important for an uncomplicated pregnancy. Although multiple observational studies have evaluated the association between thyroid dysfunction and hypertensive disorders of pregnancy, the methods and definitions of abnormalities in thyroid function tests were heterogeneous, and the results were conflicting. We aimed to examine the association between abnormalities in thyroid function tests and risk of gestational hypertension and pre-eclampsia.
Methods: In this systematic review and meta-analysis of individual-participant data, we searched MEDLINE (Ovid), Embase, Scopus, and the Cochrane Database of Systematic Reviews from date of inception to Dec 27, 2019, for prospective cohort studies with data on maternal concentrations of thyroid-stimulating hormone (TSH), free thyroxine (FT4), thyroid peroxidase (TPO) antibodies, individually or in combination, as well as on gestational hypertension, pre-eclampsia, or both. We issued open invitations to study authors to participate in the Consortium on Thyroid and Pregnancy and to share the individual-participant data. We excluded participants who had pre-existing thyroid disease or multifetal pregnancy, or were taking medications that affect thyroid function. The primary outcomes were documented gestational hypertension and pre-eclampsia. Individual-participant data were analysed using logistic mixed-effects regression models adjusting for maternal age, BMI, smoking, parity, ethnicity, and gestational age at blood sampling. The study protocol was registered with PROSPERO, CRD42019128585.
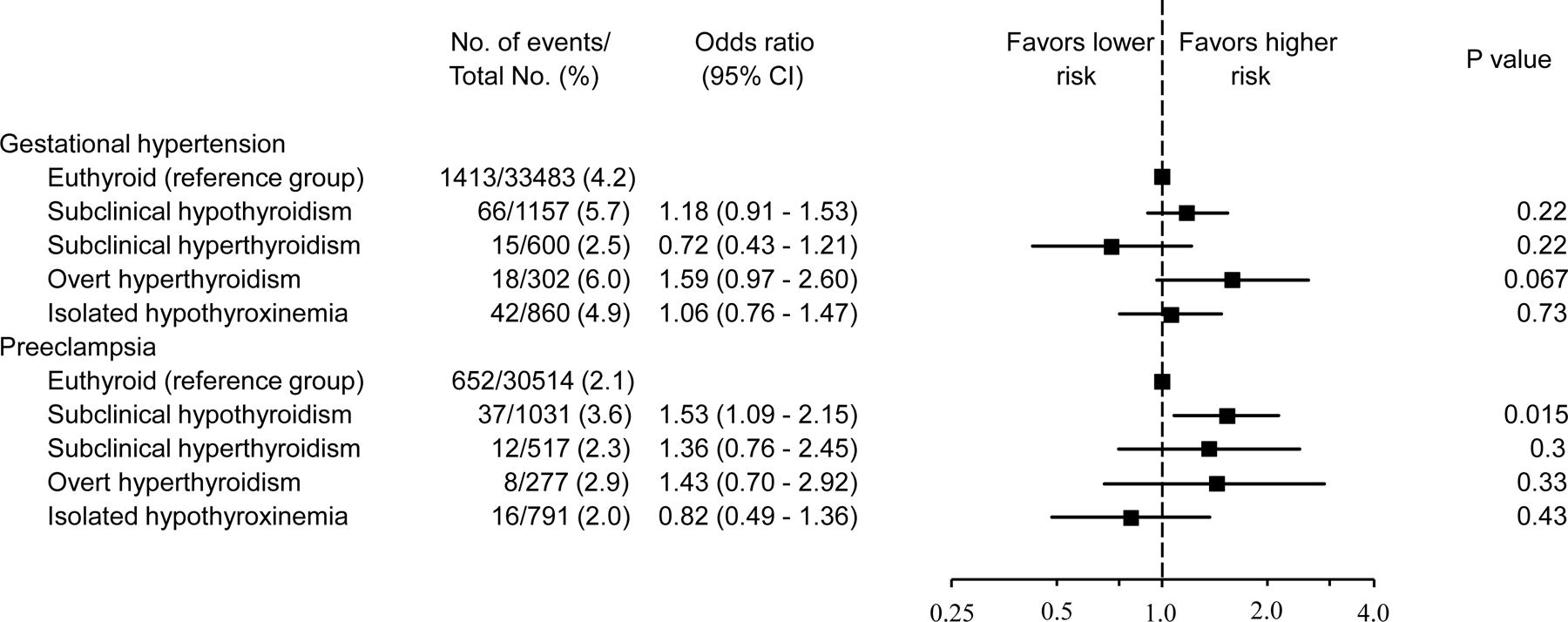
Findings: We identified 1539 published studies, of which 33 cohorts met the inclusion criteria and 19 cohorts were included after the authors agreed to participate. Our study population comprised 46 528 pregnant women, of whom 39 826 (85·6%) women had sufficient data (TSH and FT4 concentrations and TPO antibody status) to be classified according to their thyroid function status. Of these women, 1275 (3·2%) had subclinical hypothyroidism, 933 (2·3%) had isolated hypothyroxinaemia, 619 (1·6%) had subclinical hyperthyroidism, and 337 (0·8%) had overt hyperthyroidism. Compared with euthyroidism, subclinical hypothyroidism was associated with a higher risk of pre-eclampsia (2·1% vs 3·6%; OR 1·53 [95% CI 1·09-2·15]). Subclinical hyperthyroidism, isolated hypothyroxinaemia, or TPO antibody positivity were not associated with gestational hypertension or pre-eclampsia. In continuous analyses, both a higher and a lower TSH concentration were associated with a higher risk of pre-eclampsia (p=0·0001). FT4 concentrations were not associated with the outcomes measured.
Interpretation: Compared with euthyroidism, subclinical hypothyroidism during pregnancy was associated with a higher risk of pre-eclampsia. There was a U-shaped association of TSH with pre-eclampsia. These results quantify the risks of gestational hypertension or pre-eclampsia in women with thyroid function test abnormalities, adding to the total body of evidence on the risk of adverse maternal and fetal outcomes of thyroid dysfunction during pregnancy. These findings have potential implications for defining the optimal treatment target in women treated with levothyroxine during pregnancy, which needs to be assessed in future interventional studies.
Funding: Arkansas Biosciences Institute and Netherlands Organization for Scientific Research.
Copyright © 2022 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests SB declares consulting fees from Sonic Healthcare. PT reports a travel grant from Society for Endocrinology (leadership development award). EO reports grants from the National Institutes of Health. ENG received speaker's fees and payment for expert testimony from Merck and consulting fees from Brunel Rus. TGMV reports grants from the Netherlands Organization for Health Research and Development. EKA reports consultancy with Roche Diagnostics. LC received travel support by Pfizer. CD reports grants from the Chief Scientist Office (Scotland) and the British Heart Foundation. JERvL declares grant or contract support from the Dutch Heart Foundation and Amryt. SMN has received consultancy, speakers' fees, or travel support from Access Fertility, Beckman Coulter, Ferring Pharmaceuticals, Merck, Modern Fertility, Roche Diagnostics, and The Fertility Partnership. SMN also reports payments for medical–legal work and investment in The Fertility Partnership. TIMK reports lectureship fees from Berlin-Chemie, Goodlife Healthcare, Institut Biochimique SA, Merck, and Quidel. All other authors declare no competing interests.
Figures



Comment in
-
From preeclampsia to thyroid dysfunction: a long and winding road.Lancet Diabetes Endocrinol. 2022 Apr;10(4):232-233. doi: 10.1016/S2213-8587(22)00040-7. Epub 2022 Mar 4. Lancet Diabetes Endocrinol. 2022. PMID: 35255259 No abstract available.
References
-
- American College of O, Gynecologists’ Committee on Practice B-O. Gestational Hypertension and Preeclampsia: ACOG Practice Bulletin, Number 222. Obstet Gynecol 2020; 135(6): e237–e60. - PubMed
-
- Khan KS, Wojdyla D, Say L, Gulmezoglu AM, Van Look PF. WHO analysis of causes of maternal death: a systematic review. Lancet 2006; 367(9516): 1066–74. - PubMed
-
- Say L, Chou D, Gemmill A, et al. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health 2014; 2(6): e323–33. - PubMed
-
- Tranquilli AL, Dekker G, Magee L, et al. The classification, diagnosis and management of the hypertensive disorders of pregnancy: A revised statement from the ISSHP. Pregnancy Hypertens 2014; 4(2): 97–104. - PubMed
-
- Magee LA, von Dadelszen P, Bohun CM, et al. Serious perinatal complications of non-proteinuric hypertension: an international, multicentre, retrospective cohort study. J Obstet Gynaecol Can 2003; 25(5): 372–82. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
