

Dynamization-Posterior Lumbar Interbody Fusion for Hemodialysis-Related Spondyloarthropathy: Evaluation of the Radiographic Outcomes and Reoperation Rate within 2 Years Postoperatively
- PMID: 35255544
- PMCID: PMC9633239
- DOI: 10.31616/asj.2021.0312
Dynamization-Posterior Lumbar Interbody Fusion for Hemodialysis-Related Spondyloarthropathy: Evaluation of the Radiographic Outcomes and Reoperation Rate within 2 Years Postoperatively
Abstract
Study design: Clinical case series.
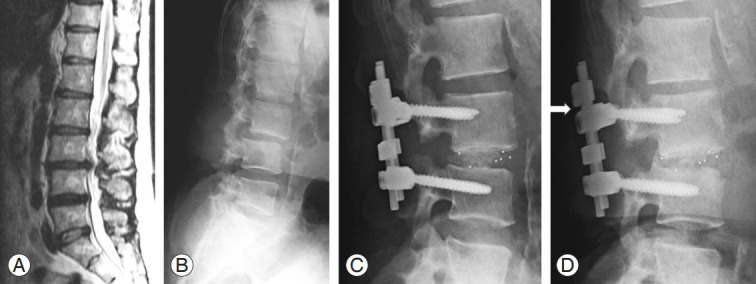
Purpose: This study aimed to report dynamization-posterior lumbar interbody fusion (PLIF), our surgical treatment for hemodialysisrelated spondyloarthropathy (HSA), and investigate patients' postoperative course within 2 years.
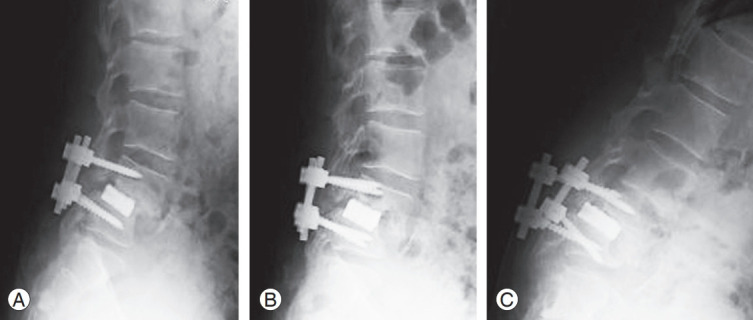
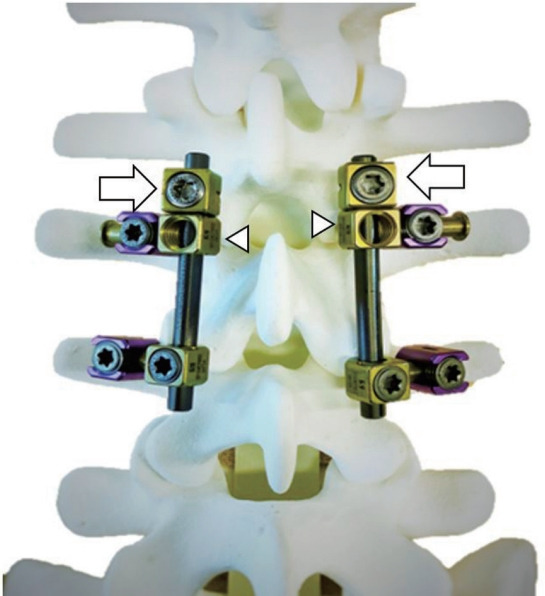
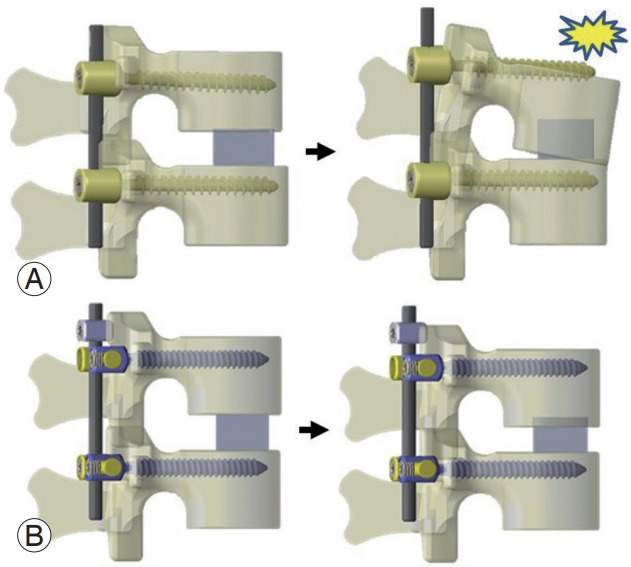
Overview of literature: HSA often requires lumbar fusion surgery. Conventional PLIF for HSA may cause progressive destructive changes in the vertebral endplate, leading to progressive cage subsidence, pedicle screw loosening, and pseudoarthrosis. A dynamic stabilization system might be effective in patients with a poor bone quality. Thus, we performed "dynamization-PLIF" in hemodialysis patients with destructive vertebral endplate changes.
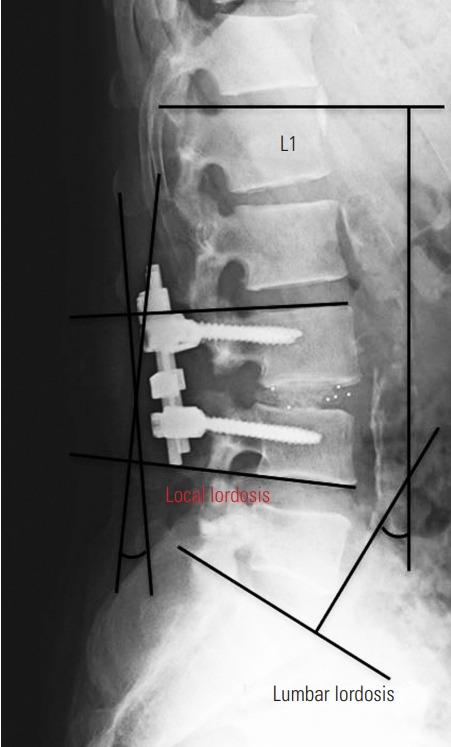
Methods: We retrospectively examined patients with HSA who underwent dynamization-PLIF at our hospital between April 2010 and March 2018. The radiographic measurements included lumbar lordosis and local lordosis in the fused segment. The evaluation points were before surgery, immediately after surgery, 1 year after surgery, and 2 years after surgery. The preoperative and postoperative radiographic findings were compared using a paired t-test. A p-value of less than 0.05 was considered significant.
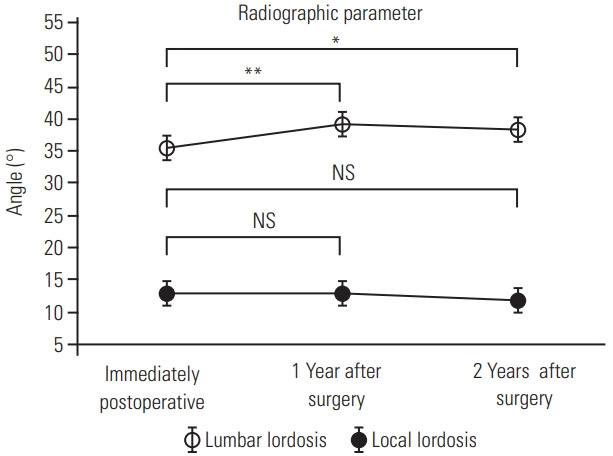
Results: We included 50 patients (28 males, 22 females). Lumbar lordosis and local lordosis were significantly improved through dynamization- PLIF (lumbar lordosis, 28.4°-35.5°; local lordosis, 2.7°-12.8°; p<0.01). The mean local lordosis was maintained throughout the postoperative course at 1- and 2-year follow-up (12.9°-12.8°, p=0.89 and 12.9°-11.8°, p=0.07, respectively). Solid fusion was achieved in 59 (89%) of 66 fused segments. Solid fusion of all fixed segments was achieved in 42 cases (84%). Within 2 years postoperatively, only six cases (12%) were reoperated (two, surgical debridement for surgical site infection; two, reoperation for pedicle screw loosening; one, laminectomy for epidural hematoma; one, additional fusion for adjacent segment disease).
Conclusions: Dynamization-PLIF showed local lordosis improvement, a high solid fusion rate, and a low reoperation rate within 2 years of follow-up.
Keywords: Destructive spondyloarthropathy; Dynamic stabilization; Dynamization; Hemodialysis; Posterior lumbar interbody fusion.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Postoperative Loss of Lumbar Lordosis Affects Clinical Outcomes in Patients with Pseudoarthrosis after Posterior Lumbar Interbody Fusion Using Cortical Bone Trajectory Screw Fixation.Asian Spine J. 2021 Jun;15(3):294-300. doi: 10.31616/asj.2020.0095. Epub 2020 Sep 22. Asian Spine J. 2021. PMID: 32951404 Free PMC article.
-
[Adjacent segment degeneration after lumbosacral fusion in spondylolisthesis: a retrospective radiological and clinical analysis].Acta Chir Orthop Traumatol Cech. 2010 Apr;77(2):124-30. Acta Chir Orthop Traumatol Cech. 2010. PMID: 20447355 Czech.
-
Influence of cage geometry on sagittal alignment in instrumented posterior lumbar interbody fusion.Spine (Phila Pa 1976). 2003 Aug 1;28(15):1693-9. doi: 10.1097/01.BRS.0000083167.78853.D5. Spine (Phila Pa 1976). 2003. PMID: 12897494
-
Lordosis Recreation in Transforaminal and Posterior Lumbar Interbody Fusion: A Cadaveric Study of the Influence of Surgical Bone Resection and Cage Angle.Spine (Phila Pa 1976). 2018 Nov 15;43(22):E1350-E1357. doi: 10.1097/BRS.0000000000002705. Spine (Phila Pa 1976). 2018. PMID: 30383726
-
Risk factors for adjacent segment degeneration after PLIF.Spine (Phila Pa 1976). 2004 Jul 15;29(14):1535-40. doi: 10.1097/01.brs.0000131417.93637.9d. Spine (Phila Pa 1976). 2004. PMID: 15247575 Review.
Cited by
-
Destructive spondyloarthropathy of the lumbar spine in patients on long-term haemodialysis: a computed tomography-based study.Eur Spine J. 2025 Jan;34(1):43-49. doi: 10.1007/s00586-024-08578-y. Epub 2024 Nov 26. Eur Spine J. 2025. PMID: 39589507
-
Two-year results of single-level fixation with lateral mass screws for cervical degenerative spondylolisthesis: patient series.J Neurosurg Case Lessons. 2023 Oct 9;6(15):CASE23343. doi: 10.3171/CASE23343. Print 2023 Oct 9. J Neurosurg Case Lessons. 2023. PMID: 37910011 Free PMC article.
-
Reoperation after short-segment lumbar spinal fusion surgery in dialysis patients: A retrospective cohort study.Medicine (Baltimore). 2024 Nov 15;103(46):e40581. doi: 10.1097/MD.0000000000040581. Medicine (Baltimore). 2024. PMID: 39560518 Free PMC article.
-
Clinical Outcomes of Lateral Lumbar Interbody Fusion with Percutaneous Pedicle Screw for Dialysis-Related Spondyloarthropathy.J Clin Med. 2024 Feb 14;13(4):1089. doi: 10.3390/jcm13041089. J Clin Med. 2024. PMID: 38398402 Free PMC article.
References
-
- Morimoto S, Nishioka H, Morita T, et al. Characteristics of 20-year survivors undergoing maintenance hemodialysis. Ther Apher Dial. 2010;14:547–51. - PubMed
-
- Maruo K, Moriyama T, Tachibana T, et al. Prognosis and adjacent segment disease after lumbar spinal fusion surgery for destructive spondyloarthropathy in long-term hemodialysis patients. J Orthop Sci. 2017;22:248–53. - PubMed
-
- Kuntz D, Naveau B, Bardin T, Drueke T, Treves R, Dryll A. Destructive spondylarthropathy in hemodialyzed patients: a new syndrome. Arthritis Rheum. 1984;27:369–75. - PubMed
-
- Fiocchi O, Bedani PL, Orzincolo C, et al. Radiological features of dialysis amyloid spondyloarthropathy. Int J Artif Organs. 1989;12:216–22. - PubMed
-
- Yamamoto T, Matsuyama Y, Tsuji T, Nakamura H, Yanase M, Ishiguro N. Destructive spondyloarthropathy in hemodialysis patients: comparison between patients with and those without destructive spondyloarthropathy. J Spinal Disord Tech. 2005;18:283–5. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
