

Updates in the treatment of vaginal cancer
- PMID: 35256422
- PMCID: PMC8921584
- DOI: 10.1136/ijgc-2021-002517
Updates in the treatment of vaginal cancer
Abstract
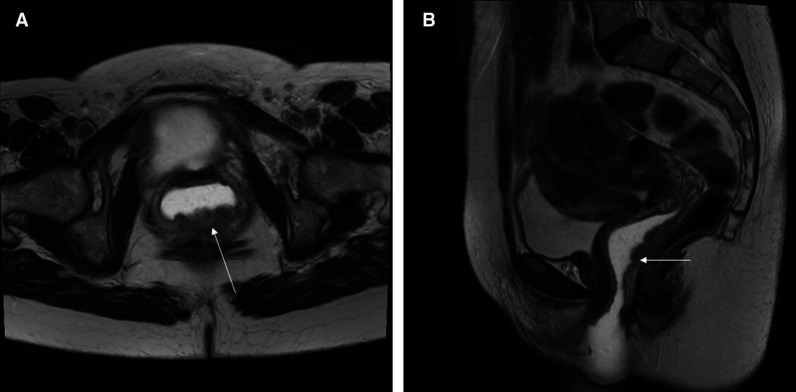
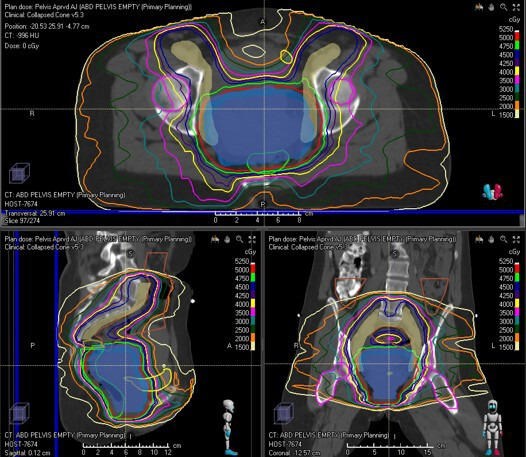
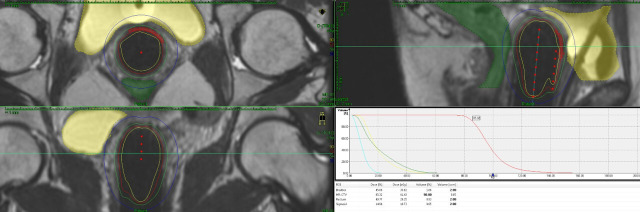
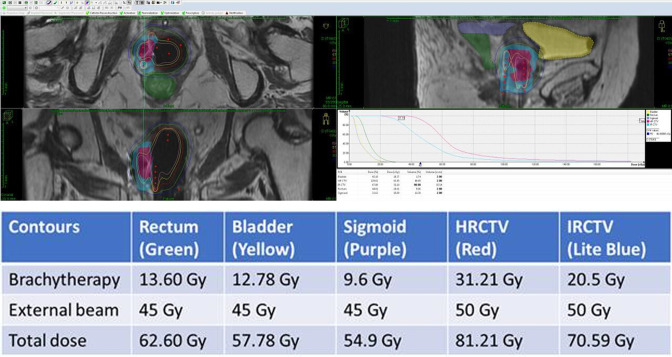
Vaginal cancer is a rare cancer. A lot of the data used in the treatment of this cancer are extrapolated from cervical cancer data. Radiation therapy plays a significant role in the treatment of vaginal cancer. The advances in radiation therapy in both external beam and brachytherapy have improved local control, survival, and toxicity. Brachytherapy plays an important role in treating vaginal cancer, but treatment should be individualized to each tumor. Imaging, particularly magnetic resonance imaging, plays an essential role in the management of patients with vaginal cancer, from diagnosis to staging to treatment management to surveillance.
Keywords: vagina; vaginal fistula; vulvar and vaginal cancer.
© IGCS and ESGO 2022. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Adhikari P, Vietje P, Mount S. Premalignant and malignant lesions of the vagina. Diagn Histopathol 2017;23:28–34. 10.1016/j.mpdhp.2016.11.006 - DOI
