

doi: 10.1016/j.eats.2021.10.018.
eCollection 2022 Mar.
Posterior Hindfoot Needle Endoscopy in the Office Setting
Affiliations
- PMID: 35256963
- PMCID: PMC8897487
- DOI: 10.1016/j.eats.2021.10.018
Item in Clipboard
Posterior Hindfoot Needle Endoscopy in the Office Setting
Arthrosc Tech.
.
Abstract
Posterior hindfoot disorders encompass a spectrum of bony, cartilaginous, and soft-tissue pathology. Traditional open surgical techniques have been increasingly replaced by less-invasive arthroscopic and endoscopic approaches. Recent innovations such as the advent of the needle arthroscope continue to push the boundary of minimally invasive interventions. This Technical Note highlights our technique for posterior hindfoot needle endoscopy for common posterior hindfoot pathologies in the wide-awake office setting, including indications, advantages, and technical pearls.
© 2021 Published by Elsevier Inc. on behalf of the Arthroscopy Association of North America.
Figures

(A) The patient is positioned prone with the foot and ankle hanging off the foot of the bed. Relevant preoperative surface anatomy markings and portal locations are indicated on a posteromedial view of the left ankle in clockwise orientation: Achilles border; medial malleolus; intermalleolar line; medial portal; lateral portal; lateral malleolus. (B) Relevant preoperative surface anatomy markings and portal locations are indicated on a posterolateral view of the left ankle.

Debridement is carried out until the intermalleolar ligament is visualized. Arthroscopic view depicts the intermalleolar ligament crossing transversely dividing the upper and lower hemispheres of a left ankle in the 4-quadrant model. The lower hemisphere allows access to the subtalar joint. The upper hemisphere grants access to the ankle joint

Four-quadrant technique for extra-articular hindfoot structures as defined by the intermalleolar ligament demonstrated on a right ankle. (1) Fibula. (2) Tibia. (3) Posterior inferior tibiofibular ligament. (4) Flexor hallucis longus tendon. (5a) Intermalleolar ligament. (5b) Superior tibial insertion of the intermalleolar ligament. (6) Tibiotalar joint. (7) Subtalar joint. (8) Posterolateral talar process. (9) Flexor hallucis longus retinaculum. (10) Calcaneofibular ligament. (11) Posterior talofibular ligament. Illustration copyright of and reproduced with permission from J.G. Kennedy, MD. (From Smyth NA, Murawski CD, Levine DS, Kennedy JG. Hindfoot arthroscopic surgery for posterior ankle impingement: A systematic surgical approach and case series. Am J Sports Med 2013;41:1869-1876.)
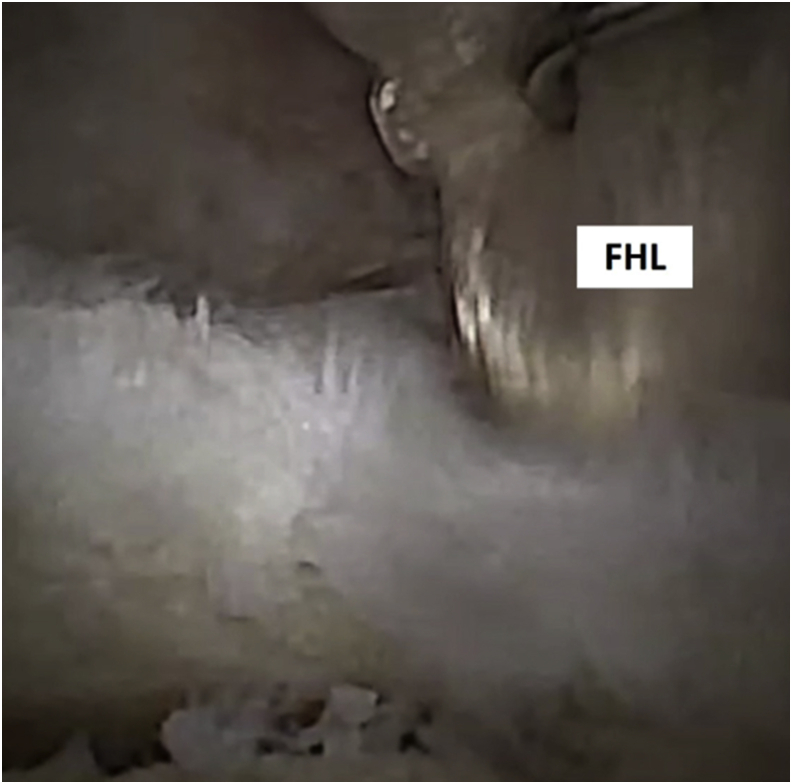
Superomedial quadrant of a left ankle demonstrating flexor hallucis longus tendon, which serves as an important landmark as it delineates the location of the neurovascular bundle, which lies medial to the FHL tendon. It is essential that all instrumentation stays in the safe zone lateral to the FHL tendon for this reason. The surgeon should be aware of the full working length of the shaver, particularly with longer blades, as the most proximal aspect of the shaver can damage the FHL tendon if not careful. The great toe may be passively flexed to aid in identification of the FHL tendon. (FHL, flexor hallucis longus.)

Inferomedial quadrant of a left ankle demonstrating intermalleolar ligament and posterolateral talar process, a location of possible Stieda lesion or os trigonum.

Trifurcation of tibial plafond, talar dome, and lateral malleolus of the tibiotalar joint of a left ankle, a typical location for osteochondral lesions. After resection of the posterior capsule, the tibiotalar joint can be visualized. Distraction of the calcaneus and dorsiflexion of ankle may be necessary for full visualization of the tibial plafond and talar dome. Osteochondral lesions, synovitis, osteophytes, hypertrophic capsule, and impingement may be identified and addressed.

Extra-articular view of subtalar joint of left ankle. After resection of the posterior capsule, the subtalar joint can be examined.
References
-
- Zwiers R., Wiegerinck J.I., Murawski C.D., Smyth N.A., Kennedy J.G., van Dijk C.N. Surgical treatment for posterior ankle impingement. Arthroscopy. 2013;29:1263–1270. - PubMed
-
- Miyamoto W., Takao M., Matsushita T. Hindfoot endoscopy for posterior ankle impingement syndrome and flexor hallucis longus tendon disorders. Foot Ankle Clin. 2015;20:139–147. - PubMed
-
- Smyth N.A., Zwiers R., Wiegerinck J.I., et al. Posterior hindfoot arthroscopy: A review. Am J Sports Med. 2014;42:225–234. - PubMed
LinkOut - more resources
Full Text Sources
