

doi: 10.1016/j.eats.2021.10.024.
eCollection 2022 Mar.
Achilles Paratenon Needle Tendoscopy in the Office Setting
Affiliations
- PMID: 35256969
- PMCID: PMC8897562
- DOI: 10.1016/j.eats.2021.10.024
Item in Clipboard
Achilles Paratenon Needle Tendoscopy in the Office Setting
Arthrosc Tech.
.
Abstract
Achilles tendinopathy is a common inflammatory condition of the Achilles tendon prevalent in the athletic population in which patients present with pain, swelling, and reduced performance exacerbated by physical activity. Operative intervention using either open or percutaneous approaches has traditionally been performed after failure of nonoperative treatment, but less invasive modalities that include endoscopic approaches have been increasingly used. This Technical Note highlights our technique for Achilles paratenon needle tendoscopy in the wide-awake office setting, with accompanying indications for use, advantages, and technical pearls.
© 2022 The Authors.
Figures
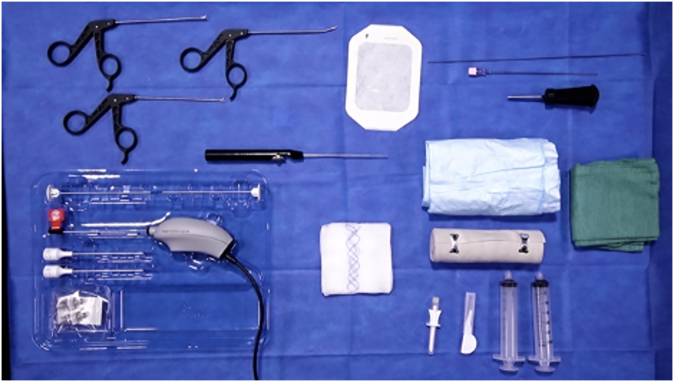
The equipment for the procedure is organized on a Mayo stand that is draped in a sterile fashion and on which this equipment is organized.
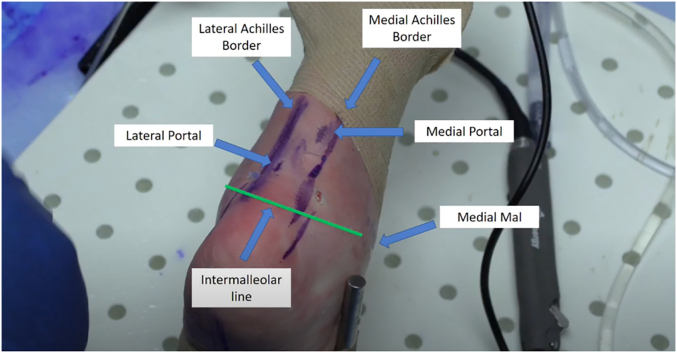
Tendoscopic approach to the left ankle with the relevant surface anatomy markings and portal locations including the Achilles borders and the intermalleolar line, with the patient in the prone position. The portal sites are made relative to the location of the presumed pathology over the Achilles tendon. Mal, malleolus.
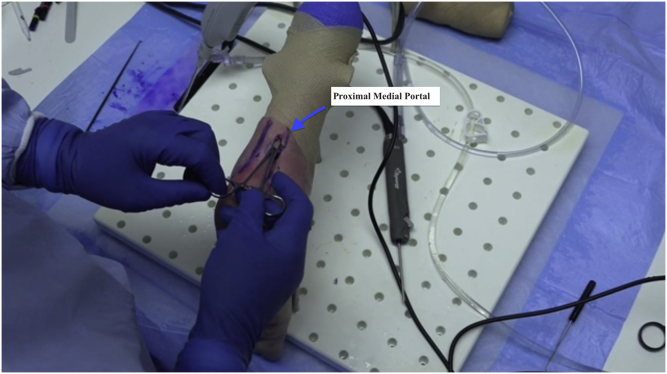
Tendoscopic approach to the left ankle via the medial portal. Typically, a proximal medial portal is made first to help visualize areas of tendinopathy.
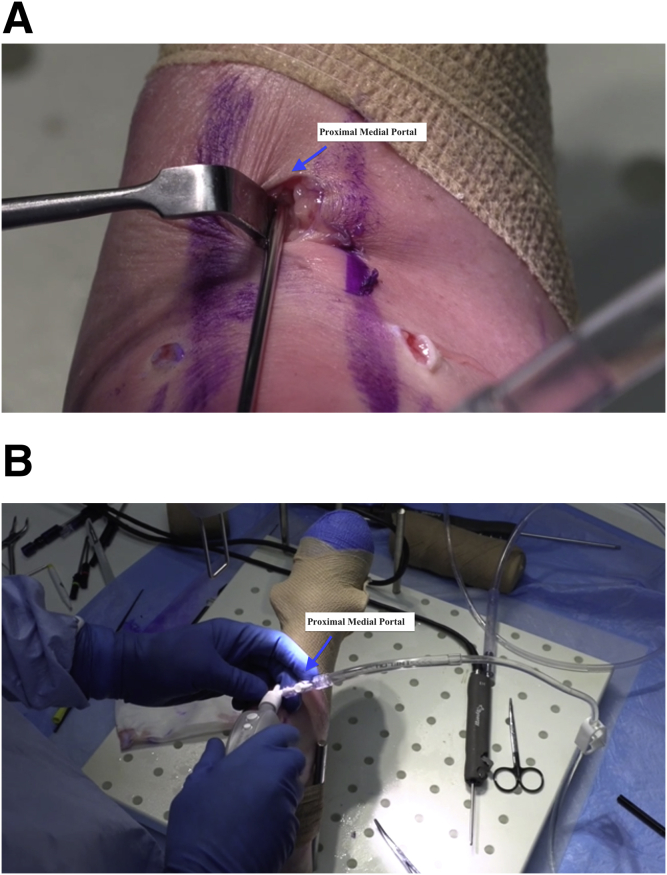
Tendoscopic approach to the left ankle via the medial portal. (A) The scope is placed between the paratenon and the Achilles tendon and subsequently advanced in a cephalad fashion. (B) The tendon and the tendon sheath are inflated, and the scope is advanced medially, laterally, and circumferentially.
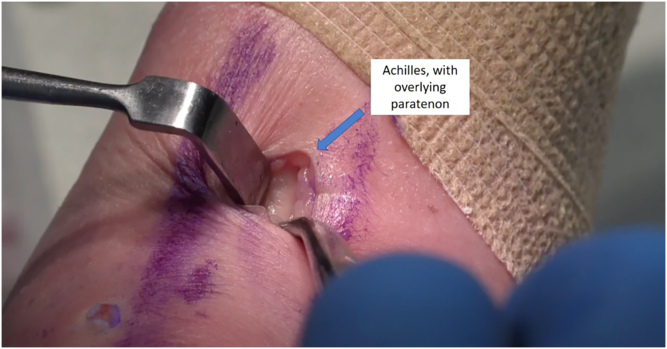
Tendoscopic approach to the left ankle via the medial portal. Blunt dissection is used to identify the paratenon layer. This layer can then be opened up sharply to access the desired space. The Achilles tendon is typically located just under the skin, so identification of the subcutaneous tissue of the paratenon should be fairly easy. The surface view of the Achilles tendon is shown, with the overlying paratenon identified.
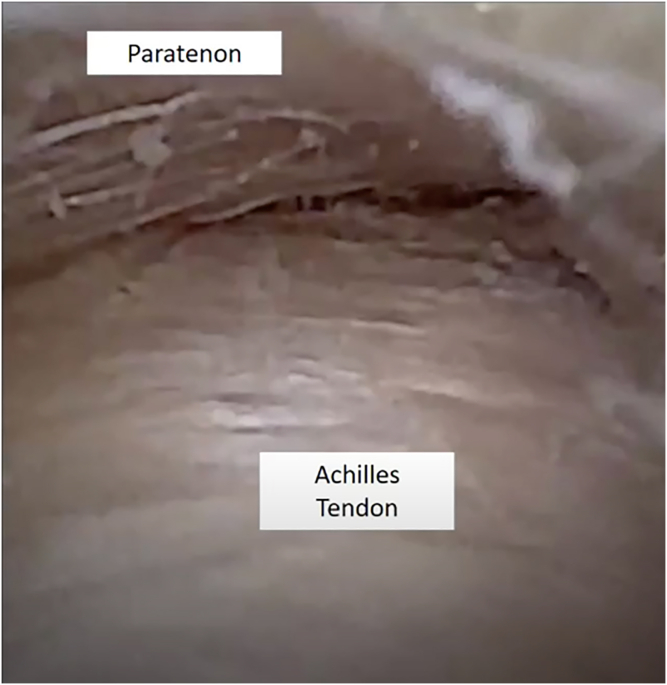
Tendoscopic approach to the left ankle via the medial portal. Once the plane established between the paratenon and the Achilles tendon is identified, the surgeon may visualize the posterior border of the Achilles tendon and the paratenon on the top of the screen.
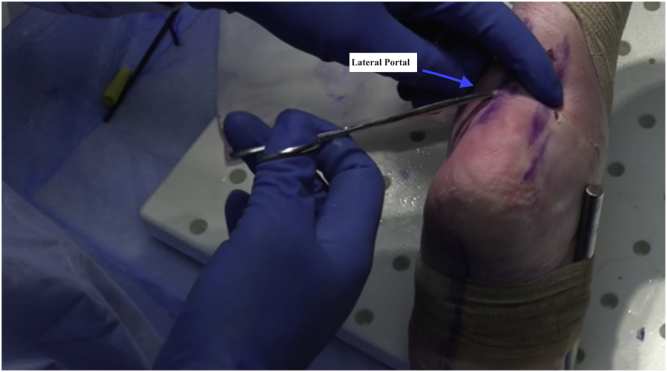
Tendoscopic approach to the left ankle via the lateral portal. A second portal site is made relative to the area of presumed pathology based on magnetic resonance imaging and direct visualization. The surgeon can use transillumination for the scope in the medial portal to help locate the portal site. Generally, one should aim to place the portals so that they flank the area of the pathology. The portals should never be made midline because the instruments will constantly interfere with one another as the surgeon converge instruments.
Tendoscopic approach to the left ankle via the lateral portal. Once the camera is through the lateral portal, the surgeon may place instrumentation through the contralateral portal and take down any visible adhesions. One must take special caution regarding the sural nerve on the lateral side because it may appear as a tendinous structure and thus may easily be mistaken for an anomalous band.
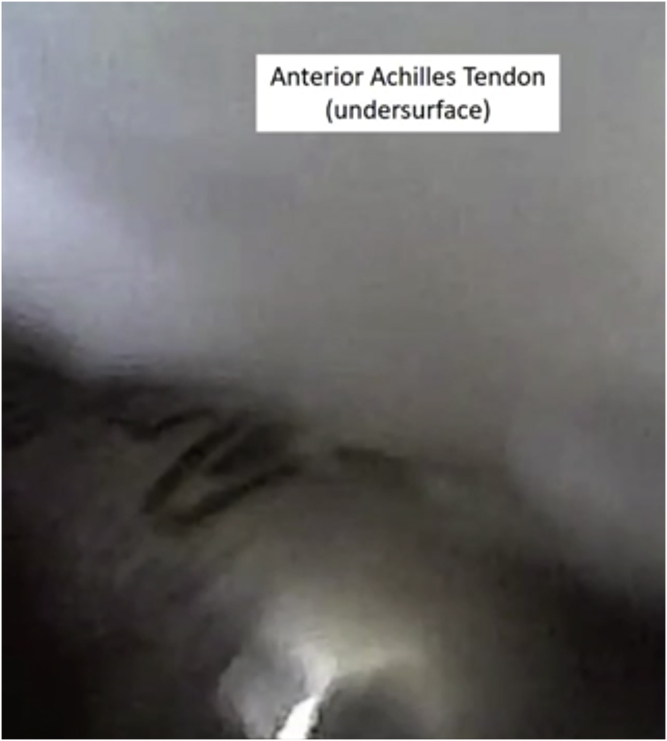
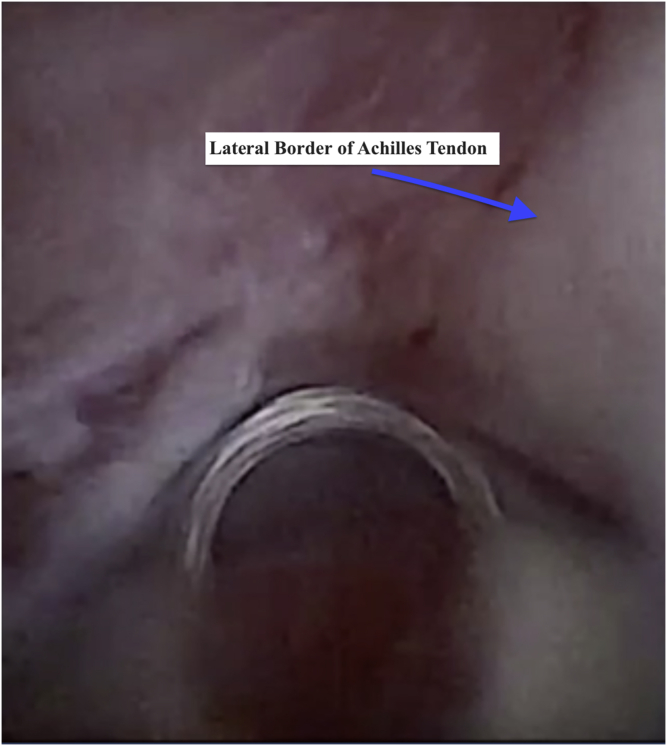
Tendoscopic approach to the left ankle via the lateral portal. After visualization of the lateral border of the Achilles and paratenon, the surgeon can use the instrumentation to proceed medially to ensure a safe distance from the sural nerve. From here, the surgeon can start addressing more superficial adhesions in the tendon and then direct the instrumentation to the undersurface of the Achilles tendon.
References
-
- Carreira D., Ballard A. Achilles tendoscopy. Foot Ankle Clin. 2015;20:27–40. - PubMed
-
- Carr A.J., Norris S.H. The blood supply of the calcaneal tendon. J Bone Joint Surg Br. 1989;71:100–101. - PubMed
-
- Gilbert P.J., Shmon C.L., Linn K.A., Singh B. Macroscopic and microvascular blood supply of the canine common calcaneal tendon. Vet Comp Orthop Traumatol. 2010;23:81–86. - PubMed
LinkOut - more resources
Full Text Sources
