

doi: 10.1016/j.eats.2021.11.004.
eCollection 2022 Mar.
Arthroscopic Bone Block Cerclage Technique Using a Tricortical Scapular Spine Autograft for Glenoid Reconstruction in Patients With Anterior Shoulder Instability
Affiliations
- PMID: 35256979
- PMCID: PMC8897580
- DOI: 10.1016/j.eats.2021.11.004
Item in Clipboard
Arthroscopic Bone Block Cerclage Technique Using a Tricortical Scapular Spine Autograft for Glenoid Reconstruction in Patients With Anterior Shoulder Instability
Arthrosc Tech.
.
Abstract
In the treatment of anterior shoulder instability with glenoid bone loss, free bone graft transfers have proven to be a viable anatomic alternative to the commonly performed, nonanatomic Latarjet procedure. Implant-free fixation of the free bone grafts, in particular, has rendered excellent short- and long-term results. However, a drawback remains the source of the graft. We describe an arthroscopic bone block cerclage technique using a tricortical scapular spine autograft, which provides an anatomic arthroscopic glenoid reconstruction with the combined benefit of sparing the subscapularis, metal-free fixation, and intraregional donor site for autograft harvesting.
© 2021 The Authors.
Figures

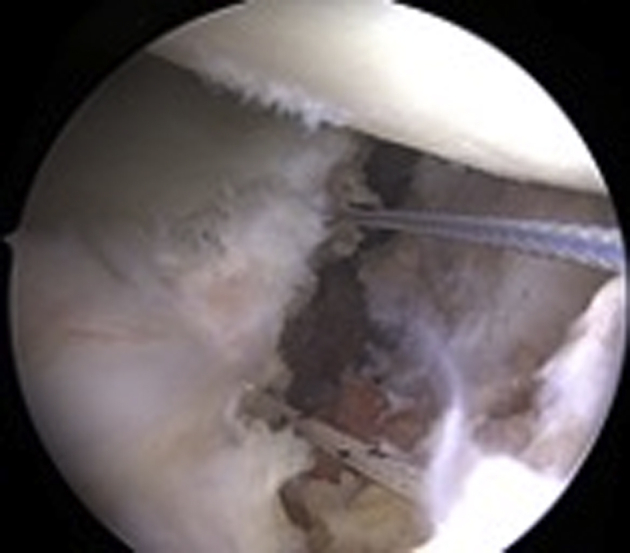
Arthroscopic view of the left shoulder from anterosuperior portal. Patient in lateral decubitus position; after mobilization of the capsulolabral complex and debridement and abrasion of the anterior glenoid defect (∗) with a motorized burr to achieve a plane surface. Note the remaining hardware (arrow) from previous stabilization surgery.

Arthroscopic view of the left shoulder from anterosuperior portal. Patient in lateral decubitus position. (A) Positioning of the drill guide from the posterior portal with the hook position 5 mm deep from the articular surface and parallel to glenoid for correct placement of the drill tunnels. (B) Intraoperative view of nitinol wires shuttled through the drill holes.
Arthroscopic view of the left shoulder from anterosuperior portal. Patient in lateral decubitus position. Exchange of nitinol wires with FiberLink (blue) and TigerLink (white) sutures for FiberTape-TigerTape Cerclage passage through glenoid and graft tunnels.

(A) Harvest location 4 to 5 cm lateral to the medial scapular border is selected, which provides the largest cross-sectional graft size while avoiding the acromial base. A horizontal incision is made along the scapular spine, and the posterior deltoid and trapezius fascia are dissected to expose the scapular spine. (B) A tricortical bone graft is harvested from a left shoulder using an oscillating saw. Patient in lateral decubitus position.
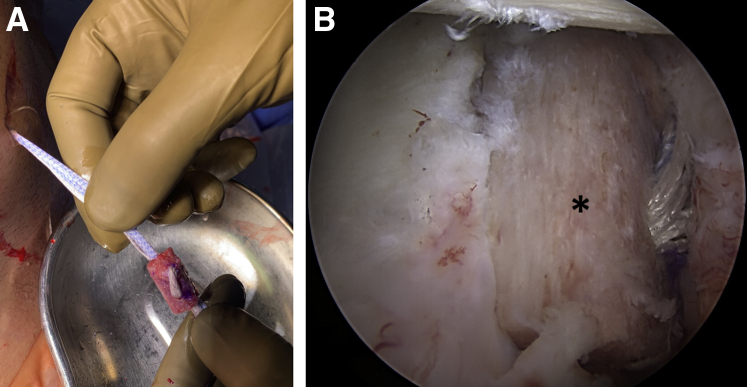
(A) Tricortical scapular spine autograft after FiberTape-TigerTape passage before insertion through the anteroinferior portal and the rotator interval. (B) Arthroscopic view of the left shoulder from anterosuperior portal after positioning of the graft (∗) on the anterior glenoid rim. Patient in lateral decubitus position.

Arthroscopic view of the left shoulder from anterosuperior portal. Patient in lateral decubitus position. Fixation of the capsulolabral complex on the native glenoid around the transferred graft with cinch stitches and knotless suture anchors (A), thus partially covering the graft (B).
References
-
- Burkhart S.S., De Beer J.F. Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: Significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion. Arthroscopy. 2000;16:677–694. - PubMed
-
- Bushnell B.D., Creighton R.A., Herring M.M. Bony instability of the shoulder. Arthroscopy. 2008;24:1061–1073. - PubMed
-
- Shah A.A., Butler R.B., Romanowski J., Goel D., Karadagli D., Warner J.J. Short-term complications of the Latarjet procedure. J Bone Joint Surg Am. 2012;94:495–501. - PubMed
-
- Degen R.M., Camp C.L., Werner B.C., Dines D.M., Dines J.S. Trends in bone-block augmentation among recently trained orthopaedic surgeons treating anterior shoulder instability. J Bone Joint Surg Am. 2016;98:e56. - PubMed
-
- Griesser M.J., Harris J.D., McCoy B.W., et al. Complications and re-operations after Bristow-Latarjet shoulder stabilization: A systematic review. J Shoulder Elbow Surg. 2013;22:286–292. - PubMed
LinkOut - more resources
Full Text Sources
