

Clinical frailty, and not features of acute infection, is associated with late mortality in COVID-19: a retrospective cohort study
- PMID: 35257497
- PMCID: PMC9088314
- DOI: 10.1002/jcsm.12966
Clinical frailty, and not features of acute infection, is associated with late mortality in COVID-19: a retrospective cohort study
Abstract
Background: Coronavirus disease 2019 (COVID-19) is associated with excess mortality after hospital discharge. Identification of patients at increased risk of death following hospital discharge is needed to guide clinical monitoring and early intervention. Herein, we aimed to identify predictors of early vs. late mortality in COVID-19 patients.
Methods: A total of 471 patients with polymerase chain reaction-confirmed COVID-19 were followed up for 9 months [median (inter-quartile range) of follow-up time: 271 (14) days] after hospital admission. COVID-19-related signs and symptoms, laboratory features, co-morbidities, Coronavirus Clinical Characterisation Consortium (4C) mortality and Clinical Frailty Scale (CFS) scores were analysed by logistic regression for association with early (28 day) vs. late mortality. Receiver operating characteristic (ROC) analysis was used to determine the discriminative value of 4C and CFS scores for early vs. late mortality.
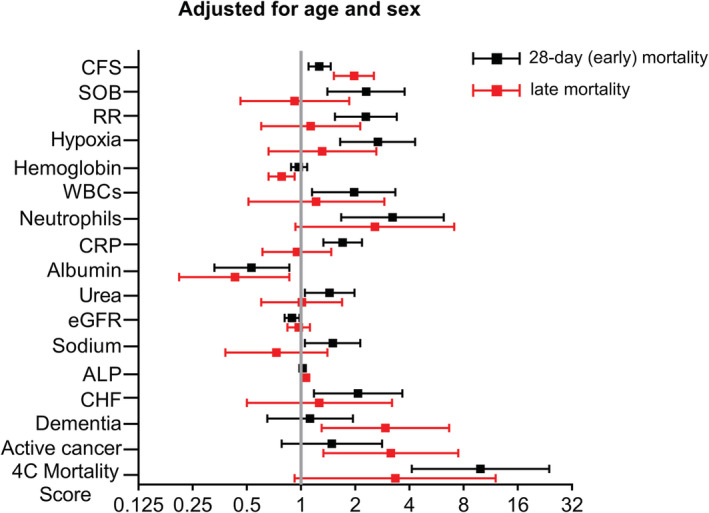
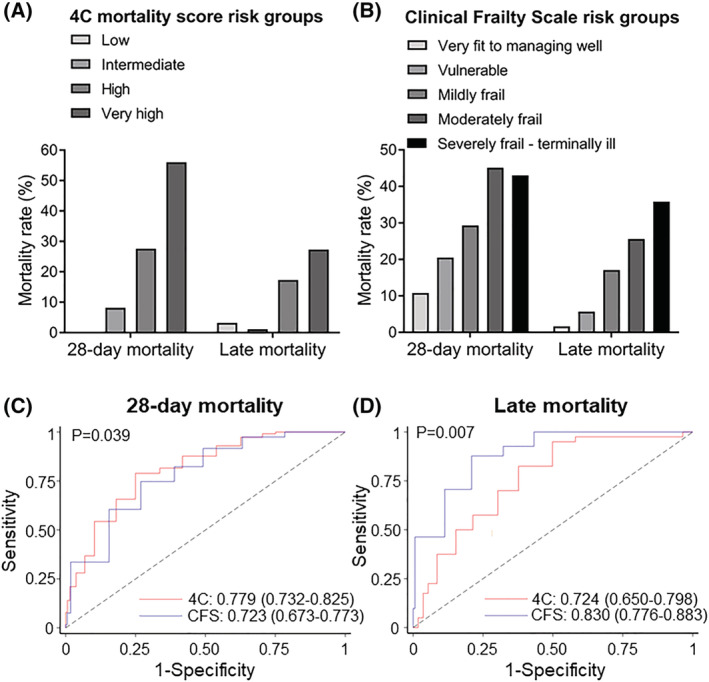
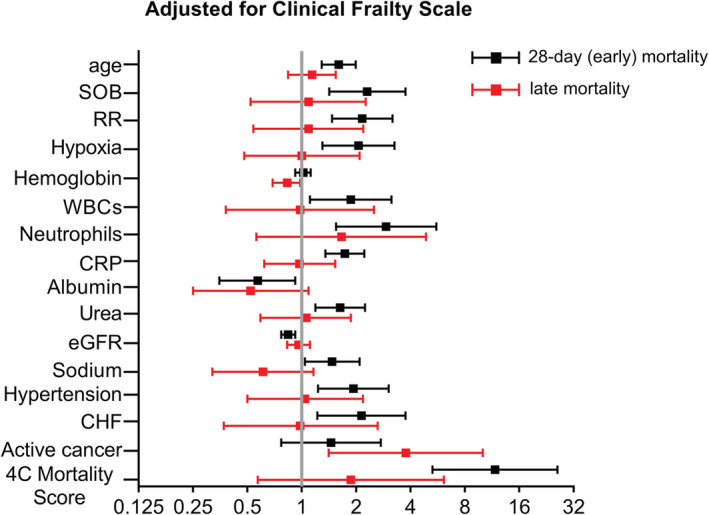
Results: A total of 120 patients died within 28 days from hospital admission. Of the remaining 351 patients, 41 died within the next 8 months. Respiratory failure, systemic inflammation, and renal impairment were associated with early mortality, while active cancer and dementia were associated with late mortality, after adjustment for age and sex. 4C mortality score and CFS were associated with both early [odds ratio (OR) (95% confidence interval-CI): 4C: 1.34 (1.25-1.45); CFS: 1.49 (1.33-1.66)] and late [OR (95% CI): 4C: 1.23 (1.12-1.36); CFS: 2.04 (1.62-2.56)] mortality. After adjustment for CFS, the association between 4C and late mortality was lost. By ROC analysis, 4C mortality score was superior to CFS for 28 day mortality [area under the curve (AUC) (95% CI): 0.779 (0.732-0.825) vs. 0.723 (0.673-0.773), respectively; P = 0.039]. In contrast, CFS had higher predictive value for late mortality compared with 4C mortality score [AUC (95% CI): 0.830 (0.776-0.883) vs. 0.724 (0.650-0.798), respectively; P = 0.007].
Conclusions: In our cohort, late mortality in COVID-19 patients is more strongly associated with premorbid clinical frailty than with severity of the acute infection phase.
Keywords: 4C mortality score; COVID-19; Frailty; Late mortality; Prognosis.
© 2022 The Authors. Journal of Cachexia, Sarcopenia and Muscle published by John Wiley & Sons Ltd on behalf of Society on Sarcopenia, Cachexia and Wasting Disorders.
Conflict of interest statement
None declared.
Figures
References
-
- World Health Organization. WHO coronavirus (COVID‐19) dashboard. https://covid19.who.int/ (Last accessed: 15 February 2022).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
