

KIR+CD8+ T cells suppress pathogenic T cells and are active in autoimmune diseases and COVID-19
- PMID: 35258337
- PMCID: PMC8995031
- DOI: 10.1126/science.abi9591
KIR+CD8+ T cells suppress pathogenic T cells and are active in autoimmune diseases and COVID-19
Abstract
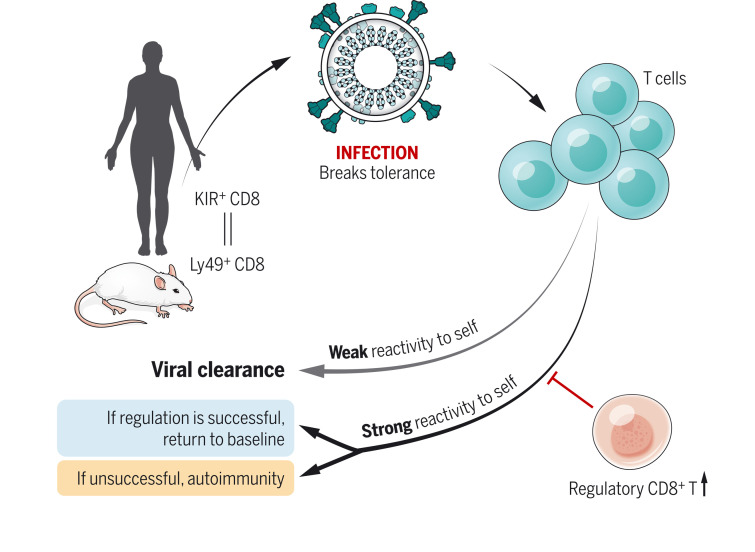
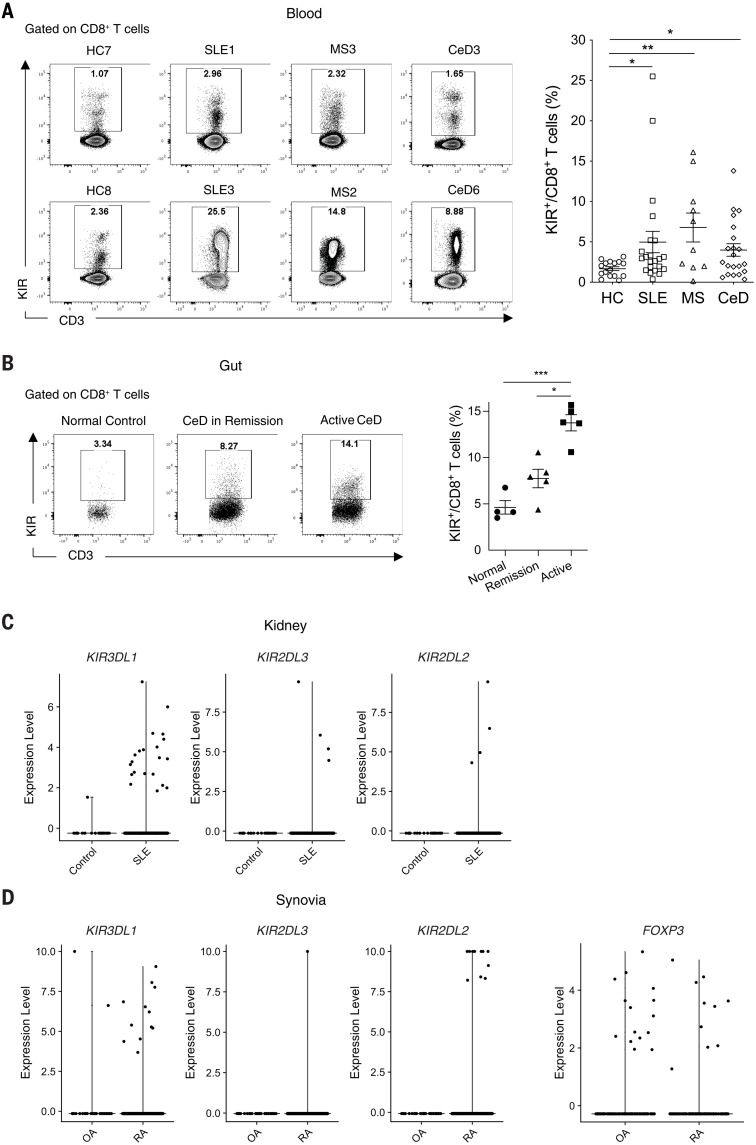
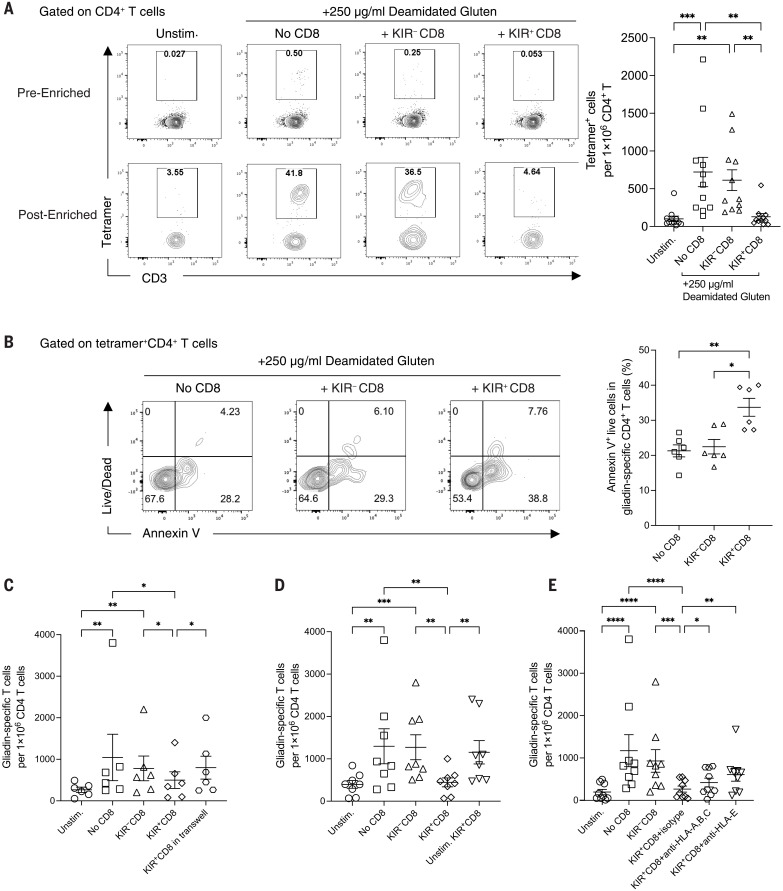
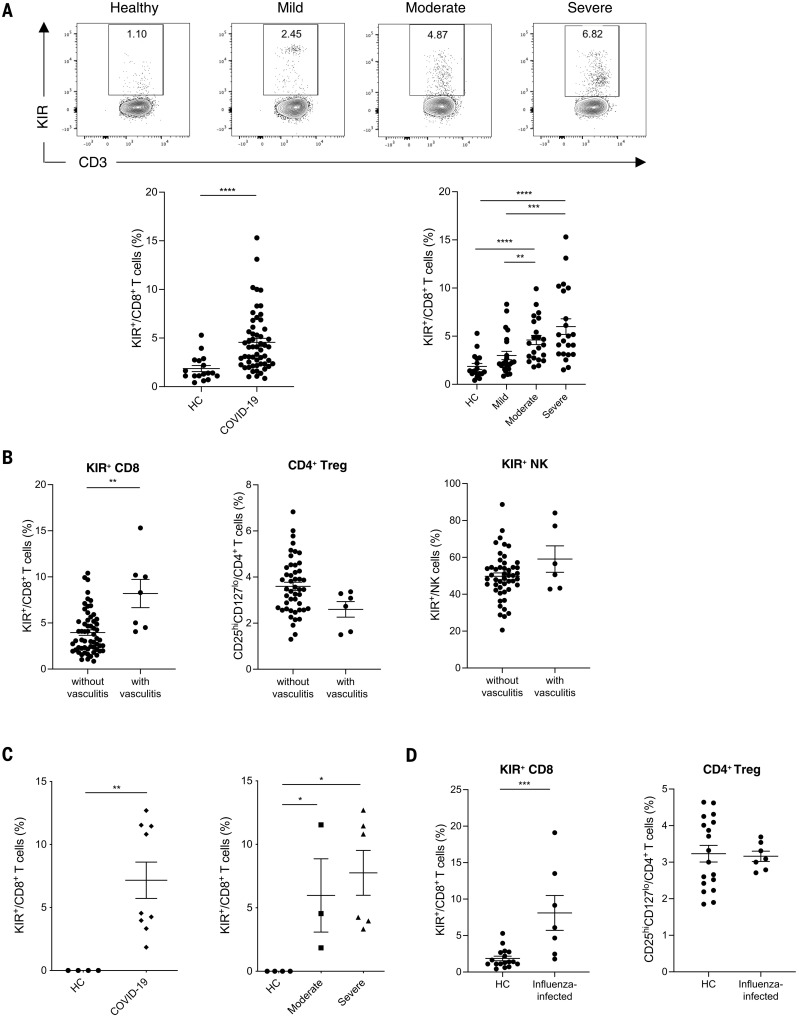
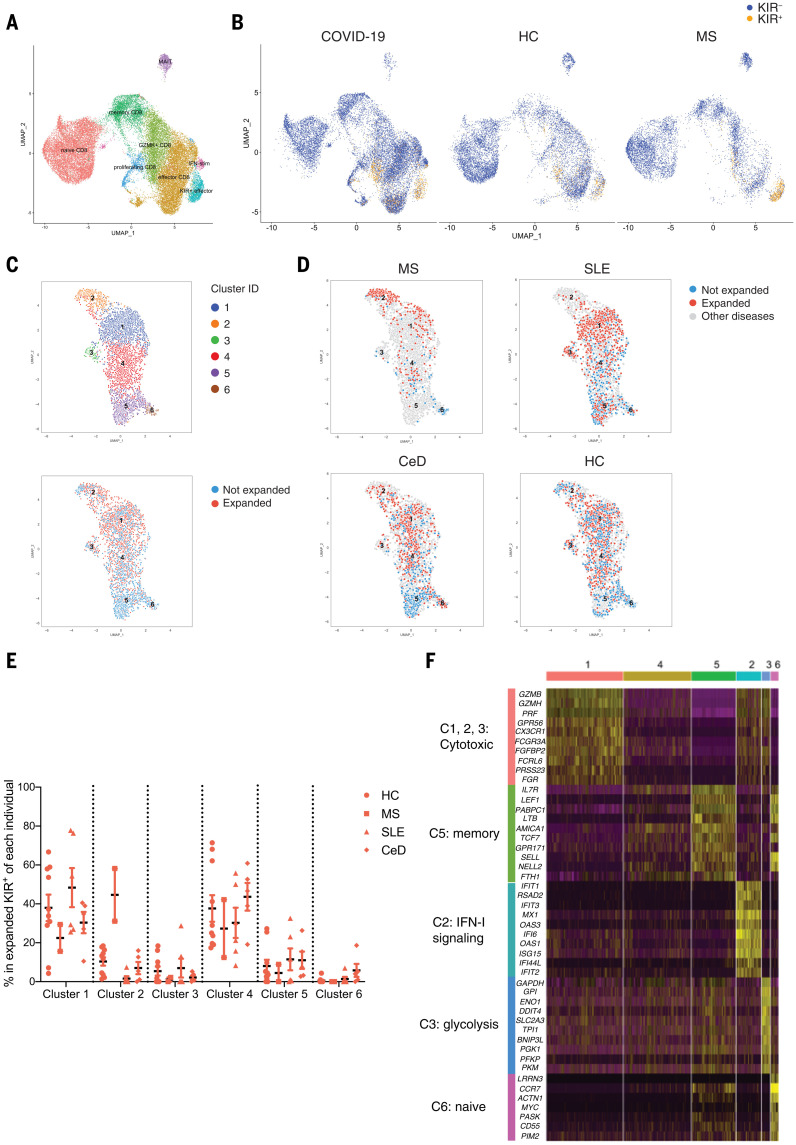
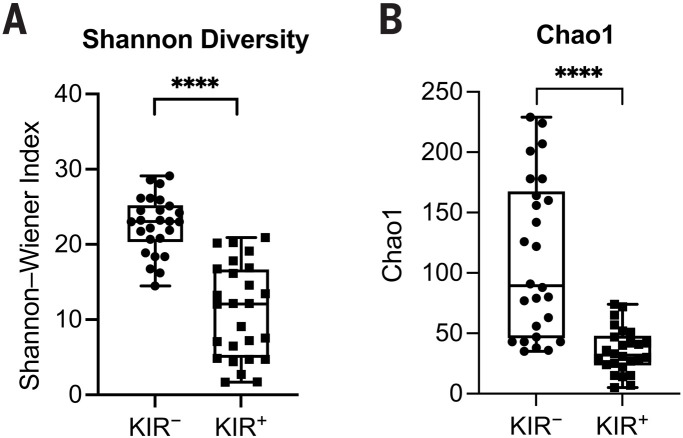
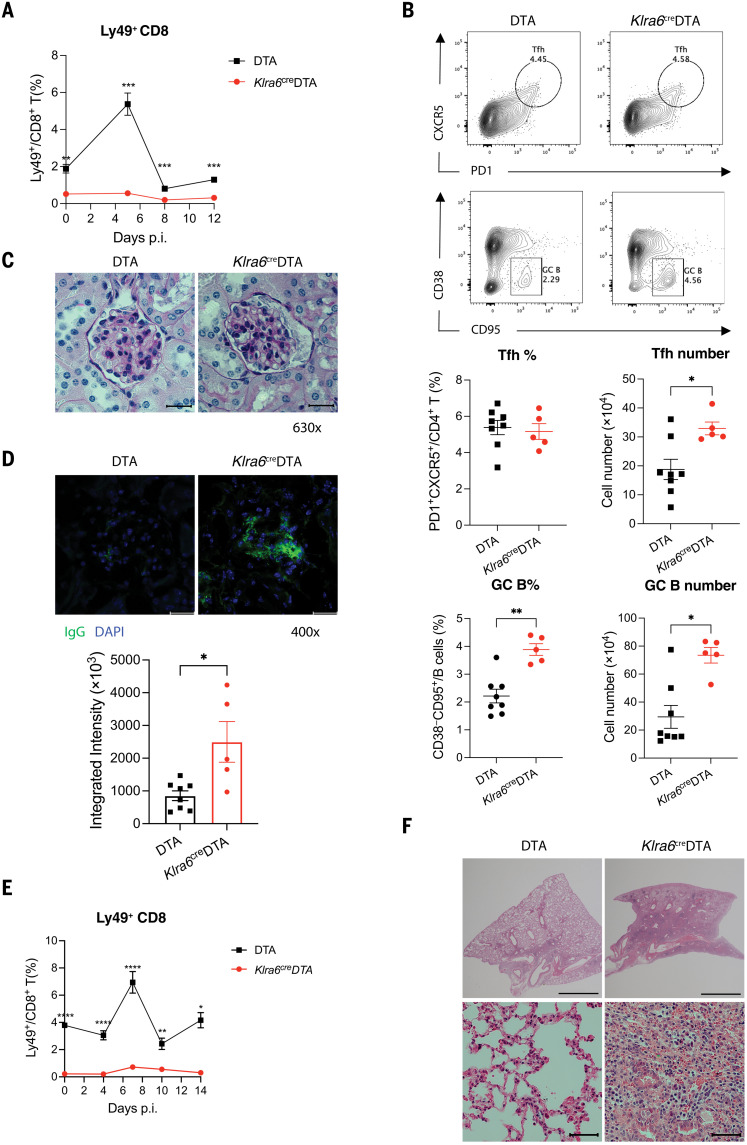
In this work, we find that CD8+ T cells expressing inhibitory killer cell immunoglobulin-like receptors (KIRs) are the human equivalent of Ly49+CD8+ regulatory T cells in mice and are increased in the blood and inflamed tissues of patients with a variety of autoimmune diseases. Moreover, these CD8+ T cells efficiently eliminated pathogenic gliadin-specific CD4+ T cells from the leukocytes of celiac disease patients in vitro. We also find elevated levels of KIR+CD8+ T cells, but not CD4+ regulatory T cells, in COVID-19 patients, correlating with disease severity and vasculitis. Selective ablation of Ly49+CD8+ T cells in virus-infected mice led to autoimmunity after infection. Our results indicate that in both species, these regulatory CD8+ T cells act specifically to suppress pathogenic T cells in autoimmune and infectious diseases.
Figures
Update of
-
Human KIR + CD8 + T cells target pathogenic T cells in Celiac disease and are active in autoimmune diseases and COVID-19.bioRxiv [Preprint]. 2021 Dec 25:2021.12.23.473930. doi: 10.1101/2021.12.23.473930. bioRxiv. 2021. Update in: Science. 2022 Apr 15;376(6590):eabi9591. doi: 10.1126/science.abi9591. PMID: 34981055 Free PMC article. Updated. Preprint.
Comment in
-
Regulatory CD8+ T cells suppress disease.Science. 2022 Apr 15;376(6590):243-244. doi: 10.1126/science.abp8243. Epub 2022 Apr 14. Science. 2022. PMID: 35420956
-
CD8+ Tregs kill pathogenic cells to avert autoimmunity.Trends Immunol. 2022 Jun;43(6):415-416. doi: 10.1016/j.it.2022.04.006. Epub 2022 May 5. Trends Immunol. 2022. PMID: 35527183
-
KIRs mark killers suppressing autoimmunity.Immunity. 2022 May 10;55(5):735-737. doi: 10.1016/j.immuni.2022.04.014. Immunity. 2022. PMID: 35545025
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
