

A Pragmatic, Stepped-Wedge, Cluster-controlled Clinical Trial of Real-Time Pneumonia Clinical Decision Support
- PMID: 35258444
- PMCID: PMC9873107
- DOI: 10.1164/rccm.202109-2092OC
A Pragmatic, Stepped-Wedge, Cluster-controlled Clinical Trial of Real-Time Pneumonia Clinical Decision Support
Abstract
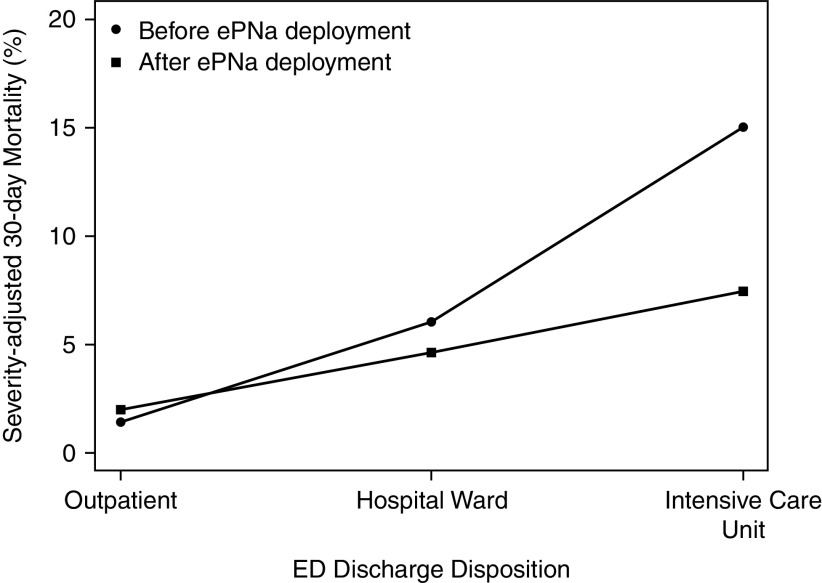
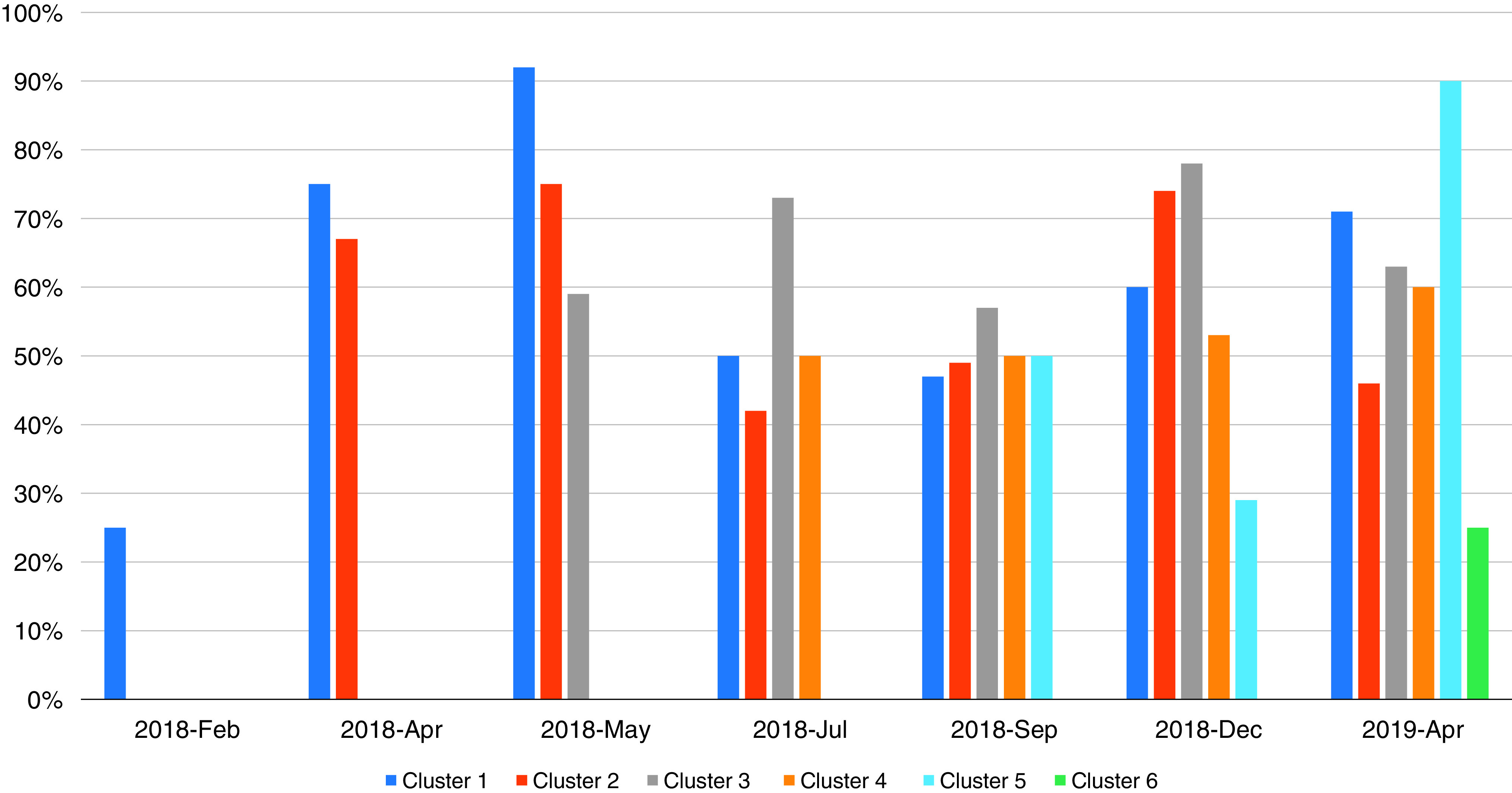
Rationale: Care of emergency department (ED) patients with pneumonia can be challenging. Clinical decision support may decrease unnecessary variation and improve care. Objectives: To report patient outcomes and processes of care after deployment of electronic pneumonia clinical decision support (ePNa): a comprehensive, open loop, real-time clinical decision support embedded within the electronic health record. Methods: We conducted a pragmatic, stepped-wedge, cluster-controlled trial with deployment at 2-month intervals in 16 community hospitals. ePNa extracts real-time and historical data to guide diagnosis, risk stratification, microbiological studies, site of care, and antibiotic therapy. We included all adult ED patients with pneumonia over the course of 3 years identified by International Classification of Diseases, 10th Revision discharge coding confirmed by chest imaging. Measurements and Main Results: The median age of the 6,848 patients was 67 years (interquartile range, 50-79), and 48% were female; 64.8% were hospital admitted. Unadjusted mortality was 8.6% before and 4.8% after deployment. A mixed effects logistic regression model adjusting for severity of illness with hospital cluster as the random effect showed an adjusted odds ratio of 0.62 (0.49-0.79; P < 0.001) for 30-day all-cause mortality after deployment. Lower mortality was consistent across hospital clusters. ePNa-concordant antibiotic prescribing increased from 83.5% to 90.2% (P < 0.001). The mean time from ED admission to first antibiotic was 159.4 (156.9-161.9) minutes at baseline and 150.9 (144.1-157.8) minutes after deployment (P < 0.001). Outpatient disposition from the ED increased from 29.2% to 46.9%, whereas 7-day secondary hospital admission was unchanged (5.2% vs. 6.1%). ePNa was used by ED clinicians in 67% of eligible patients. Conclusions: ePNa deployment was associated with improved processes of care and lower mortality. Clinical trial registered with www.clinicaltrials.gov (NCT03358342).
Keywords: antibiotic use; clinical decision support; emergency department; mortality; pneumonia.
Figures

Comment in
-
Can Electronic Decision Support Tools Really Reduce Mortality from Community-acquired Pneumonia?Am J Respir Crit Care Med. 2022 Jun 1;205(11):1267-1268. doi: 10.1164/rccm.202202-0358ED. Am J Respir Crit Care Med. 2022. PMID: 35320063 Free PMC article. No abstract available.
References
-
- Ramirez JA, Wiemken TL, Peyrani P, Arnold FW, Kelley R, Mattingly WA, et al. University of Louisville Pneumonia Study Group Adults hospitalized with pneumonia in the United States: incidence, epidemiology, and mortality. Clin Infect Dis . 2017;65:1806–1812. - PubMed
-
- Niederman MS, Luna CM. Community-acquired pneumonia guidelines: a global perspective. Semin Respir Crit Care Med . 2012;33:298–310. - PubMed
-
- McMahon LF, Jr, Wolfe RA, Tedeschi PJ. Variation in hospital admissions among small areas. A comparison of Maine and Michigan. Med Care . 1989;27:623–631. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
