

Predictive Accuracy of a Perioperative Laboratory Test-Based Prediction Model for Moderate to Severe Acute Kidney Injury After Cardiac Surgery
- PMID: 35258532
- PMCID: PMC8905398
- DOI: 10.1001/jama.2022.1751
Predictive Accuracy of a Perioperative Laboratory Test-Based Prediction Model for Moderate to Severe Acute Kidney Injury After Cardiac Surgery
Abstract
Importance: Effective treatment of acute kidney injury (AKI) is predicated on timely diagnosis; however, the lag in the increase in serum creatinine levels after kidney injury may delay therapy initiation.
Objective: To determine the derivation and validation of predictive models for AKI after cardiac surgery.
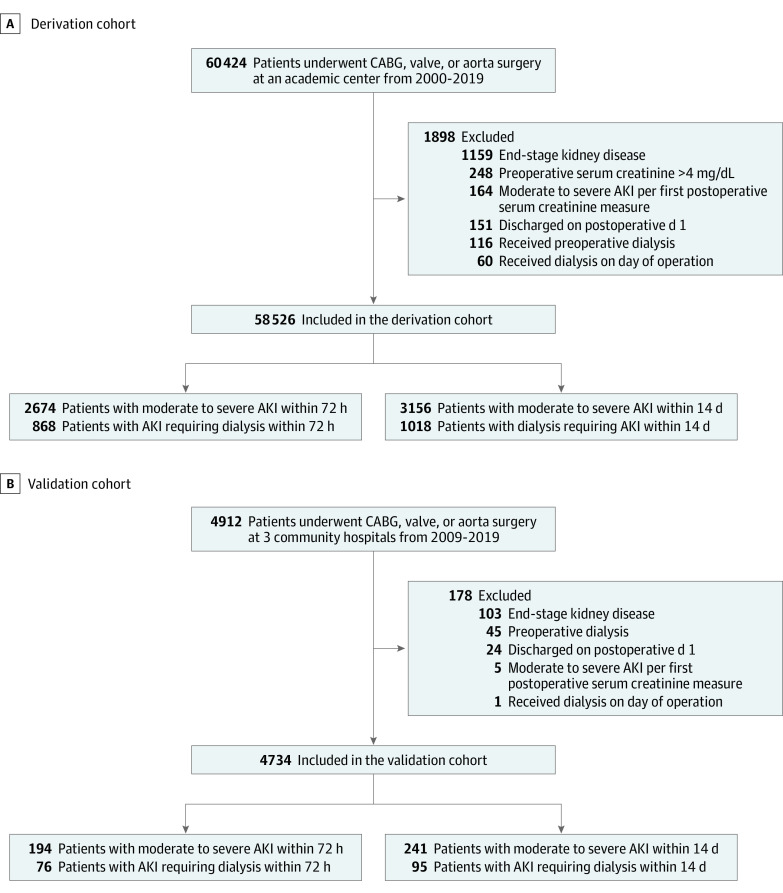
Design, setting, and participants: Multivariable prediction models were derived based on a retrospective observational cohort of adult patients undergoing cardiac surgery between January 2000 and December 2019 from a US academic medical center (n = 58 526) and subsequently validated on an external cohort from 3 US community hospitals (n = 4734). The date of final follow-up was January 15, 2020.
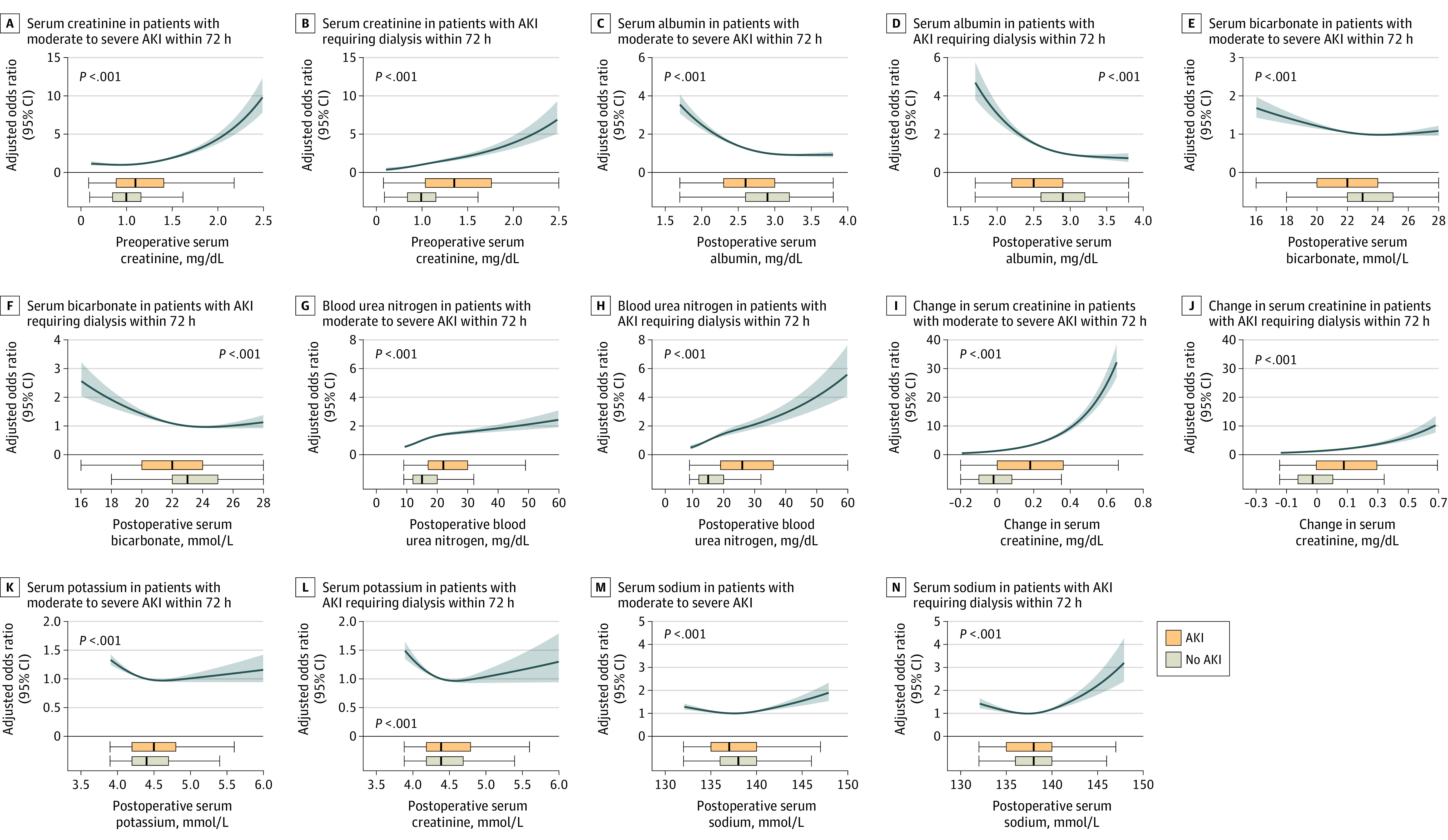
Exposures: Perioperative change in serum creatinine and postoperative blood urea nitrogen, serum sodium, potassium, bicarbonate, and albumin from the first metabolic panel after cardiac surgery.
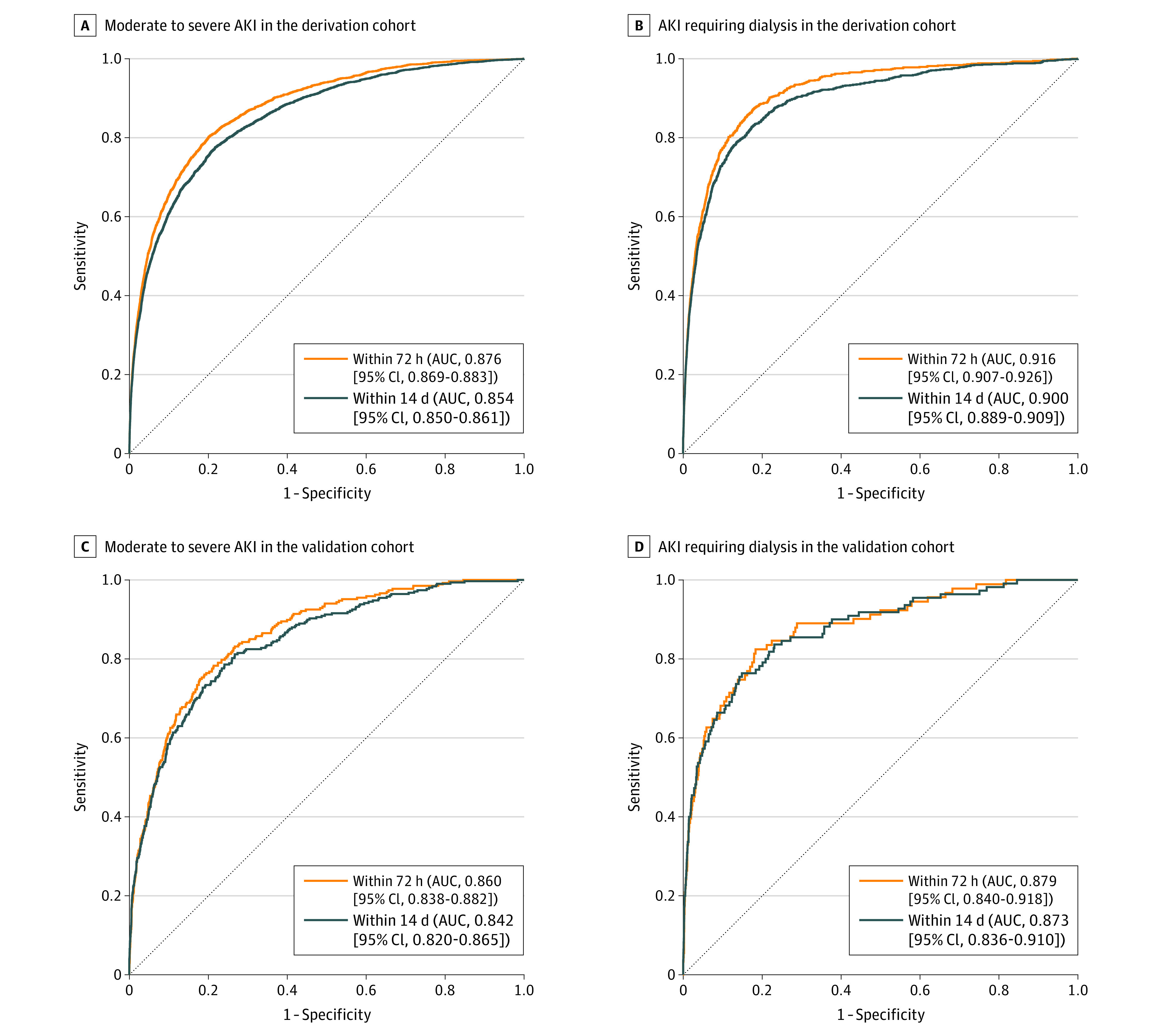
Main outcomes and measures: Area under the receiver-operating characteristic curve (AUC) and calibration measures for moderate to severe AKI, per Kidney Disease: Improving Global Outcomes (KDIGO), and AKI requiring dialysis prediction models within 72 hours and 14 days following surgery.
Results: In a derivation cohort of 58 526 patients (median [IQR] age, 66 [56-74] years; 39 173 [67%] men; 51 503 [91%] White participants), the rates of moderate to severe AKI and AKIrequiring dialysis were 2674 (4.6%) and 868 (1.48%) within 72 hours and 3156 (5.4%) and 1018 (1.74%) within 14 days after surgery. The median (IQR) interval to first metabolic panel from conclusion of the surgical procedure was 10 (7-12) hours. In the derivation cohort, the metabolic panel-based models had excellent predictive discrimination for moderate to severe AKI within 72 hours (AUC, 0.876 [95% CI, 0.869-0.883]) and 14 days (AUC, 0.854 [95% CI, 0.850-0.861]) after the surgical procedure and for AKI requiring dialysis within 72 hours (AUC, 0.916 [95% CI, 0.907-0.926]) and 14 days (AUC, 0.900 [95% CI, 0.889-0.909]) after the surgical procedure. In the validation cohort of 4734 patients (median [IQR] age, 67 (60-74) years; 3361 [71%] men; 3977 [87%] White participants), the models for moderate to severe AKI after the surgical procedure showed AUCs of 0.860 (95% CI, 0.838-0.882) within 72 hours and 0.842 (95% CI, 0.820-0.865) within 14 days and the models for AKI requiring dialysis and 14 days had an AUC of 0.879 (95% CI, 0.840-0.918) within 72 hours and 0.873 (95% CI, 0.836-0.910) within 14 days after the surgical procedure. Calibration assessed by Spiegelhalter z test showed P >.05 indicating adequate calibration for both validation and derivation models.
Conclusions and relevance: Among patients undergoing cardiac surgery, a prediction model based on perioperative basic metabolic panel laboratory values demonstrated good predictive accuracy for moderate to severe acute kidney injury within 72 hours and 14 days after the surgical procedure. Further research is needed to determine whether use of the risk prediction tool improves clinical outcomes.
Conflict of interest statement
Figures
Comment in
-
Predictive Models for Acute Kidney Injury Following Cardiac Surgery: The Importance of Accurate and Actionable Prediction.JAMA. 2022 Mar 8;327(10):927-929. doi: 10.1001/jama.2022.1823. JAMA. 2022. PMID: 35258544 No abstract available.
References
-
- Zarbock A, Küllmar M, Ostermann M, et al. . Prevention of cardiac surgery-associated acute kidney injury by implementing the KDIGO guidelines in high-risk patients identified by biomarkers: the PrevAKI-multicenter randomized controlled trial. Anesth Analg. 2021;133(2):292-302. doi:10.1213/ANE.0000000000005458 - DOI - PubMed
