

National differences in implementation of minimally invasive surgery for colorectal cancer and the influence on short-term outcomes
- PMID: 35258664
- PMCID: PMC9283170
- DOI: 10.1007/s00464-021-08974-1
National differences in implementation of minimally invasive surgery for colorectal cancer and the influence on short-term outcomes
Abstract
Background: The timing and degree of implementation of minimally invasive surgery (MIS) for colorectal cancer vary among countries. Insights in national differences regarding implementation of new surgical techniques and the effect on postoperative outcomes are important for quality assurance, can show potential areas for country-specific improvement, and might be illustrative and supportive for similar implementation programs in other countries. Therefore, this study aimed to evaluate differences in patient selection, applied techniques, and results of minimal invasive surgery for colorectal cancer between the Netherlands and Sweden.
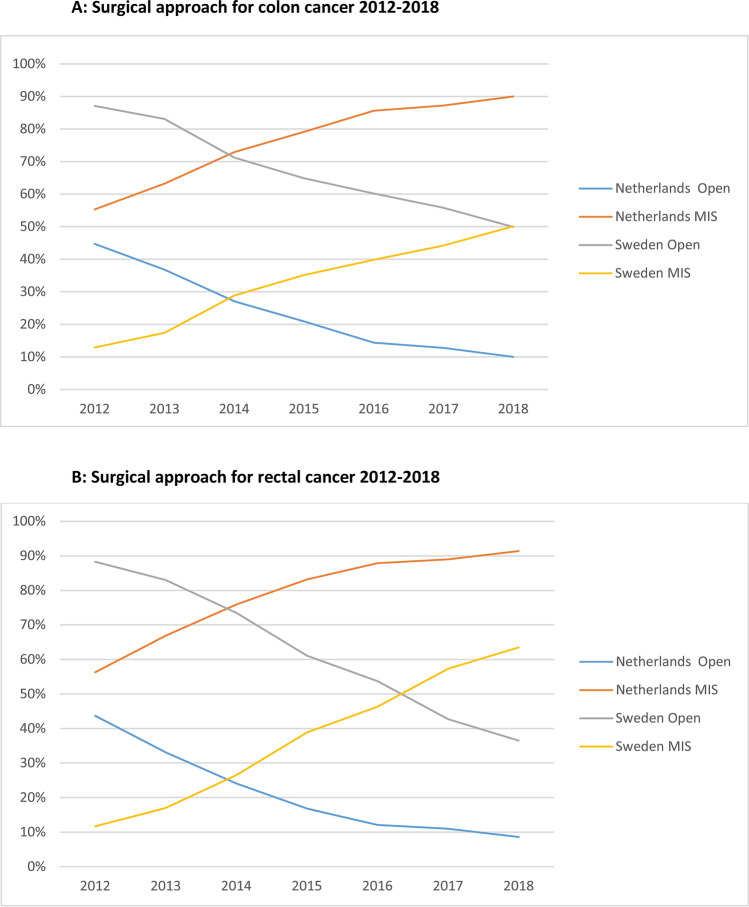
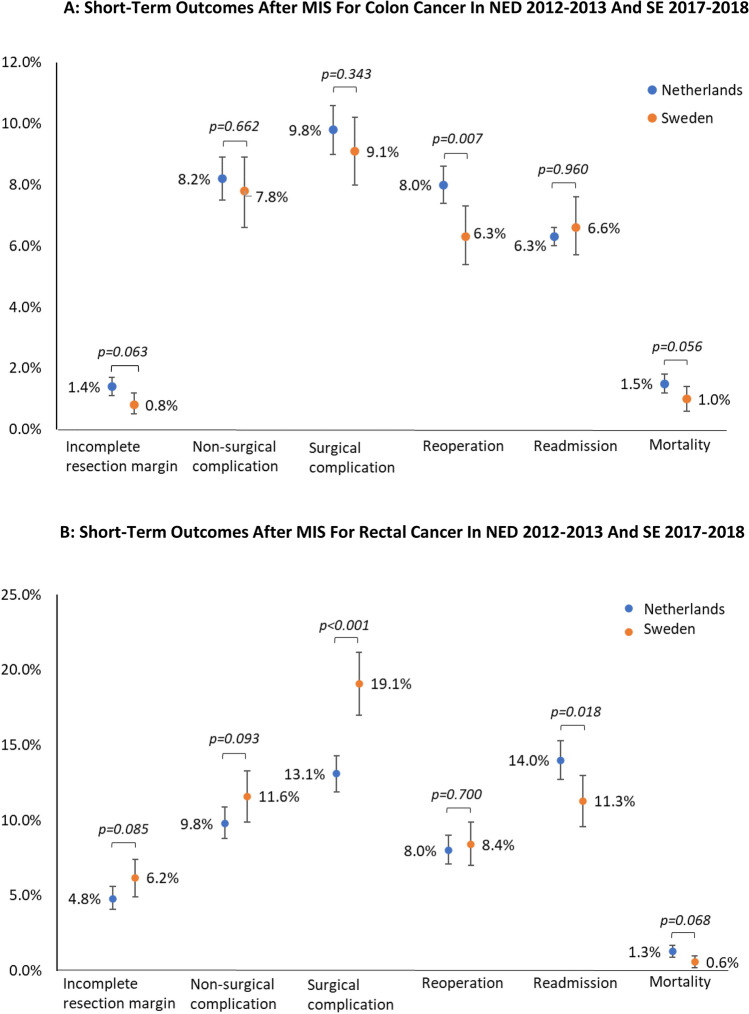
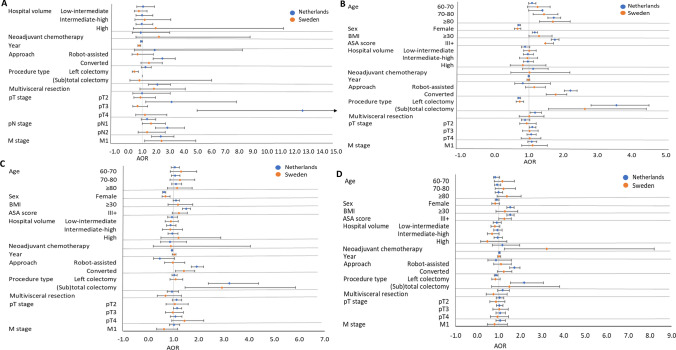
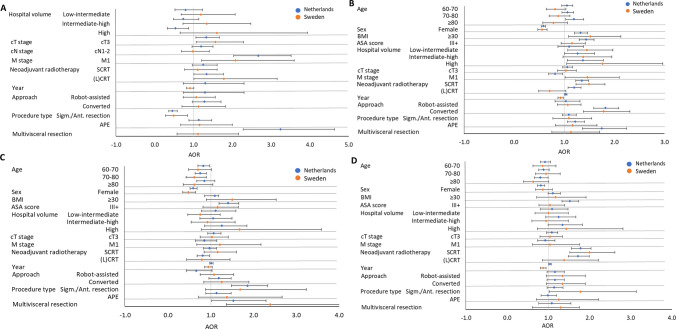
Methods: Patients who underwent elective minimally invasive surgery for T1-3 colon or rectal cancer (2012-2018) registered in the Dutch ColoRectal Audit or Swedish ColoRectal Cancer Registry were included. Time trends in the application of MIS were determined. Outcomes were compared for time periods with a similar level of MIS implementation (Netherlands 2012-2013 versus Sweden 2017-2018). Multilevel analyses were performed to identify factors associated with adverse short-term outcomes.
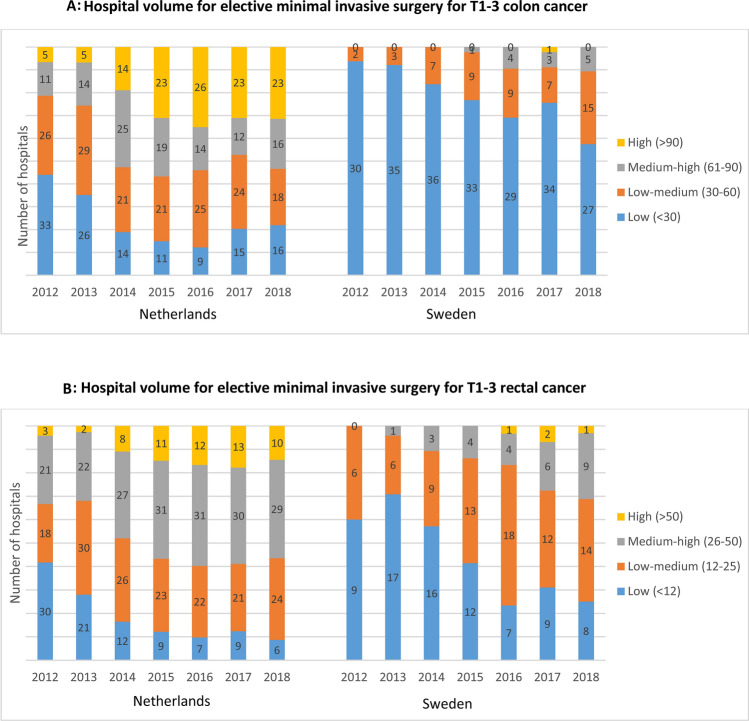
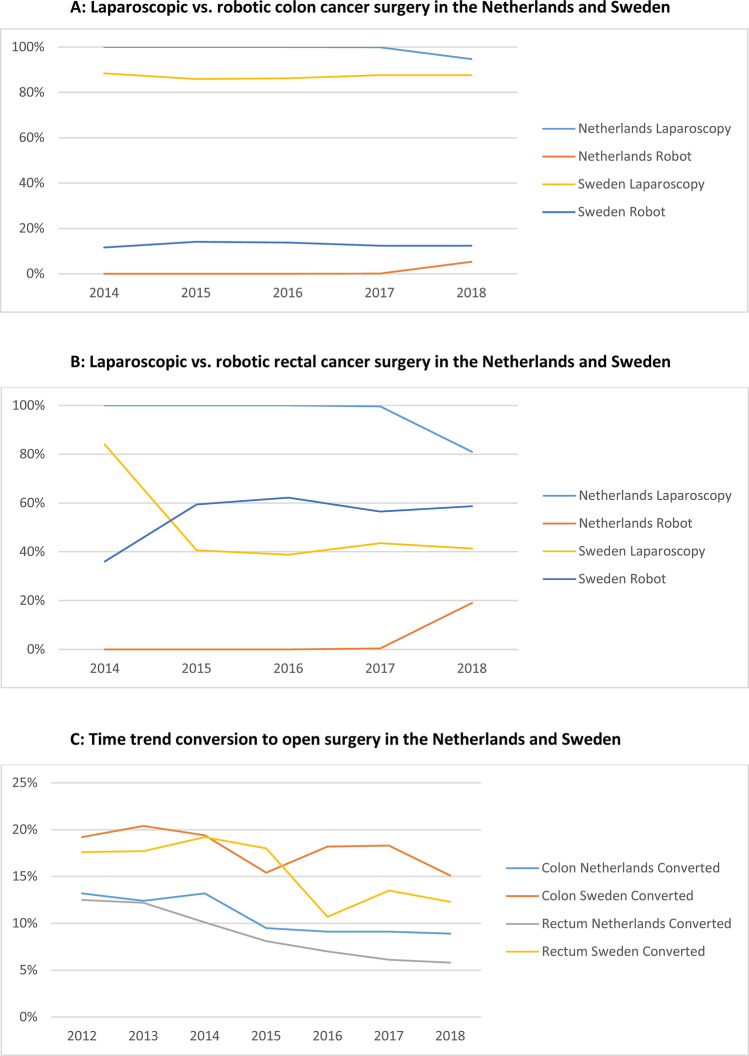
Results: A total of 46,095 Dutch and 8,819 Swedish patients undergoing MIS for colorectal cancer were included. In Sweden, MIS implementation was approximately 5 years later than in the Netherlands, with more robotic surgery and lower volumes per hospital. Although conversion rates were higher in Sweden, oncological and surgical outcomes were comparable. MIS in the Netherlands for the years 2012-2013 resulted in a higher reoperation rate for colon cancer and a higher readmission rate but lower non-surgical complication rates for rectal cancer if compared with MIS in Sweden during 2017-2018.
Conclusion: This study showed that the implementation of MIS for colorectal cancer occurred later in Sweden than the Netherlands, with comparable outcomes despite lower volumes. Our study demonstrates that new surgical techniques can be implemented at a national level in a controlled and safe way, with thorough quality assurance.
Keywords: Colorectal cancer; Hospital volume; Laparoscopy; Minimal invasive surgery; Robotic surgery; Short-term outcomes.
© 2022. The Author(s).
Conflict of interest statement
Anne-Loes K. Warps, Marinke Westerterp, Robin Detering, Annika Sjövall, Anna Martling, Jan Willem T. Dekker, Rob A.E.M. Tollenaar, Peter Matthiessen, and Pieter J. Tanis have no conflicts of interests and financial ties to disclose. Deborah Saraste has no conflicts of interests to disclose, but received funding from the foundation Serafimerlasarettet and the Bengt Ihre Foundation.
Figures
References
-
- de Neree tot Babberich MPM, Detering R, Dekker JWT, Elferink MA, Tollenaar RAEM, Wouters MWJM, Tanis PJ, Beets-Tan RGH, Bemelman WA, Boerma D, Coenen PP, Dekker E, Eddes EH, Gelderblom H, van der Harst E, Karsten TM, van Krieken JH, van Leersum NJ, Lemmens VE, Meijerink WJ, Manusama ER, Marijnen CAM, Nagtegaal ID, van de Velde CJ, Wiggers T. Achievements in colorectal cancer care during 8 years of auditing in The Netherlands. Eur J Surg Oncol. 2018;44:1361–1370. doi: 10.1016/j.ejso.2018.06.001. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
