

The effect of continuous intercostal nerve block vs. single shot on analgesic outcomes and hospital stays in minimally invasive direct coronary artery bypass surgery: a retrospective cohort study
- PMID: 35260084
- PMCID: PMC8903669
- DOI: 10.1186/s12871-022-01607-7
The effect of continuous intercostal nerve block vs. single shot on analgesic outcomes and hospital stays in minimally invasive direct coronary artery bypass surgery: a retrospective cohort study
Abstract
Background: Minimally invasive direct coronary artery bypass (MIDCAB) grafting surgery is accompanied by severe pain. Although continuous intercostal nerve block (CINB) has become one of the multimodal analgesic techniques in single port thoracoscopic surgery, its effects on MIDCAB are unclear. The purpose of this study was to compare the effects of CINB and single shot on analgesic outcomes and hospital stays in patients undergoing MIDCAB in a real-world setting.
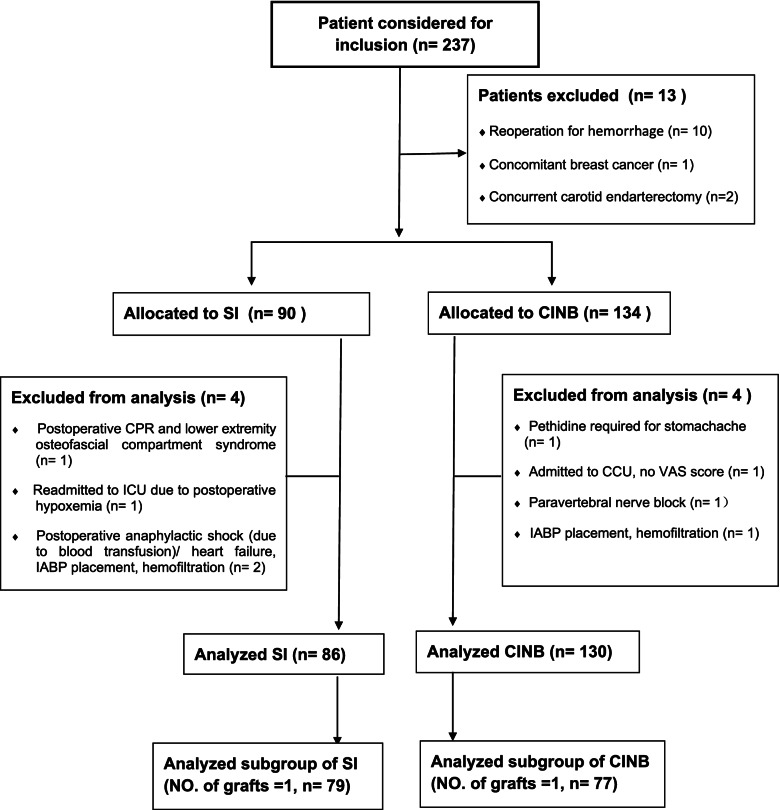
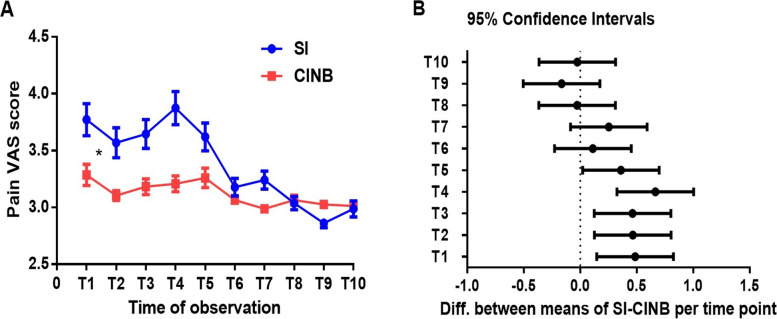
Methods: A retrospective cohort study was carried out at Peking University Third Hospital, China. Two hundred and sixteen patients undergoing MIDCAB were divided into two groups: a CINB group and a single block (SI) group. The primary outcome was postoperative maximal visual analog scale (VAS); secondary outcomes included the number of patients with maximal VAS ≤ 3, the demand for and consumed doses of pethidine and tramadol, and the length of intensive care unit (ICU) and hospital stays. The above data and the area under the VAS curve in the 70 h after extubation for the two subgroups (No. of grafts = 1) were also compared.
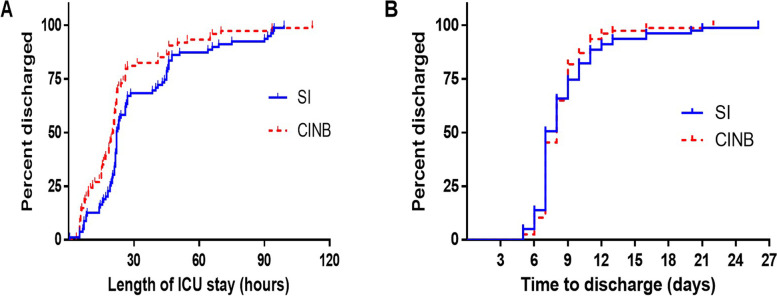
Results: The maximum VAS was lower in the CINB group, and there were more cases with maximum VAS ≤ 3 in the CINB group: CINB 52 (40%) vs. SI 17 (20%), P = 0.002. The percentage of cases requiring tramadol and pethidine was less in CINB, P = 0.001. Among all patients, drug doses were significantly lower in the CINB group [tramadol: CINB 0 (0-100) mg vs. SI 100 (0-225) mg, P = 0.0001; pethidine: CINB 0 (0-25) mg vs. SI 25 (0-50) mg, P = 0.0004]. Further subgroup analysis showed that the area under the VAS curve in CINB was smaller: 28.05 in CINB vs. 30.41 in SI, P = 0.002. Finally, the length of ICU stay was shorter in CINB than in SI: 20.5 (11.3-26.0) h vs. 22.0 (19.0-45.0) h, P = 0.011.
Conclusions: CINB is associated with decreased demand for rescue analgesics and shorter length of ICU stay when compared to single shot intercostal nerve block. Additional randomized controlled trial (RCT) is needed to support these findings.
Keywords: Block; Coronary artery bypass; Intercostal nerve; Length of stay; Minimally invasive surgery; Outcomes.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Kettering K, Dapunt O, Baer FM. Minimally invasive direct coronary artery bypass grafting: a systematic review. J Cardiovasc Surg (Torino) 2004;45(3):255–264. - PubMed
-
- Menkis AH, Martin J, Cheng DC, Fitzgerald DC, Freedman JJ, Gao C, Koster A, Mackenzie GS, Murphy GJ, Spiess B, et al. Drug, devices, technologies, and techniques for blood management in minimally invasive and conventional cardiothoracic surgery: a consensus statement from the International Society for Minimally Invasive Cardiothoracic Surgery (ISMICS) 2011. Innovations (Phila) 2012;7(4):229–241. doi: 10.1097/imi.0b013e3182747699. - DOI - PubMed
-
- Rogers CA, Pike K, Angelini GD, Reeves BC, Glauber M, Ferrarini M, Murphy GJ. An open randomized controlled trial of median sternotomy versus anterolateral left thoracotomy on morbidity and health care resource use in patients having off-pump coronary artery bypass surgery: the Sternotomy Versus Thoracotomy (STET) trial. J Thorac Cardiovasc Surg. 2013;146(2):306–16 e1–9. doi: 10.1016/j.jtcvs.2012.04.020. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
