

A faecal microbiota signature with high specificity for pancreatic cancer
- PMID: 35260444
- PMCID: PMC9185815
- DOI: 10.1136/gutjnl-2021-324755
A faecal microbiota signature with high specificity for pancreatic cancer
Abstract
Background: Recent evidence suggests a role for the microbiome in pancreatic ductal adenocarcinoma (PDAC) aetiology and progression.
Objective: To explore the faecal and salivary microbiota as potential diagnostic biomarkers.
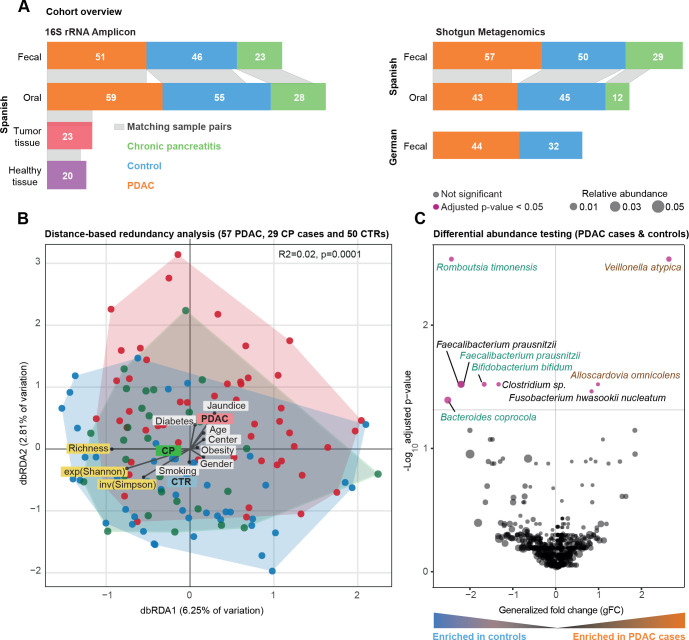
Methods: We applied shotgun metagenomic and 16S rRNA amplicon sequencing to samples from a Spanish case-control study (n=136), including 57 cases, 50 controls, and 29 patients with chronic pancreatitis in the discovery phase, and from a German case-control study (n=76), in the validation phase.
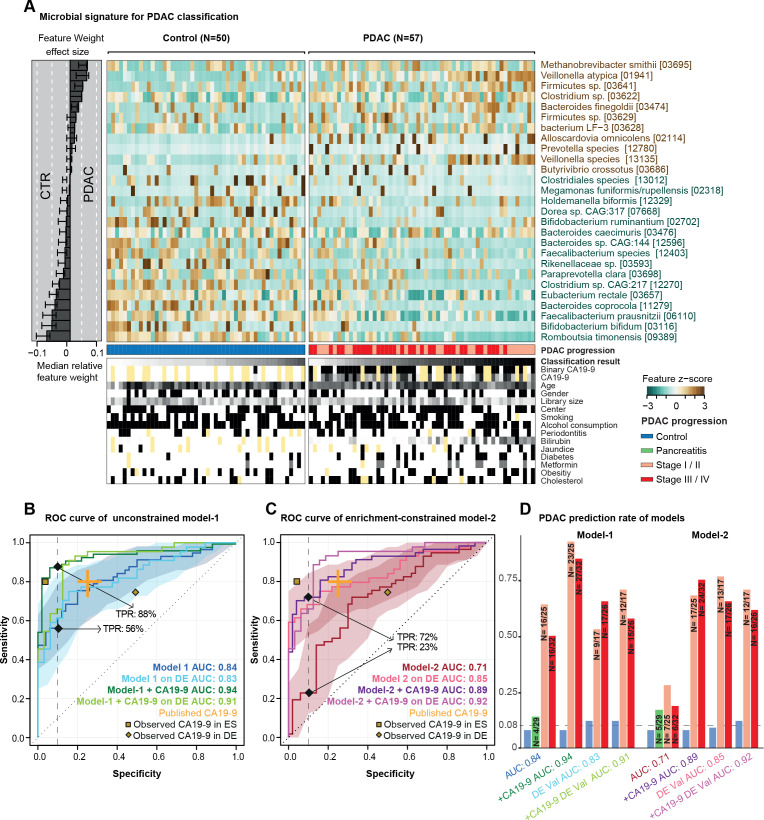
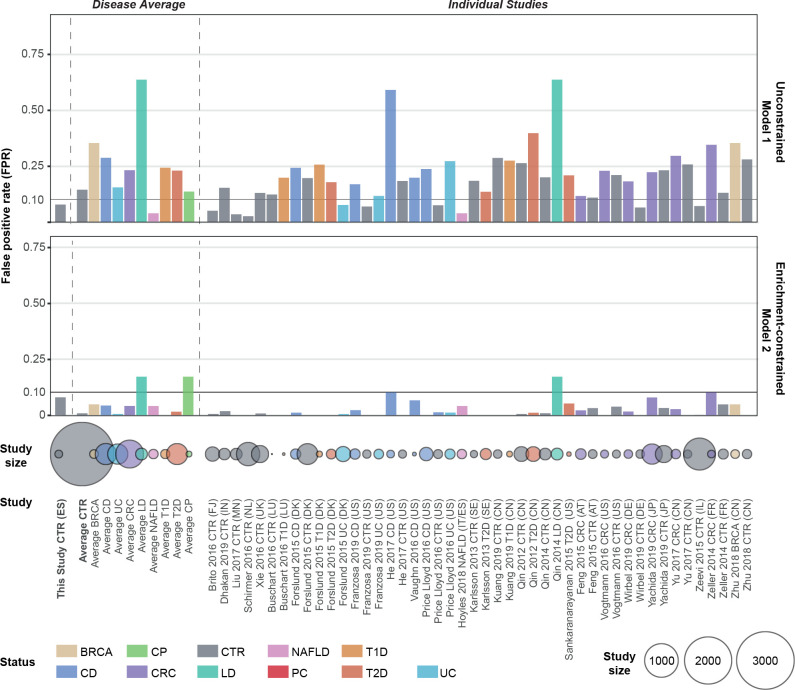
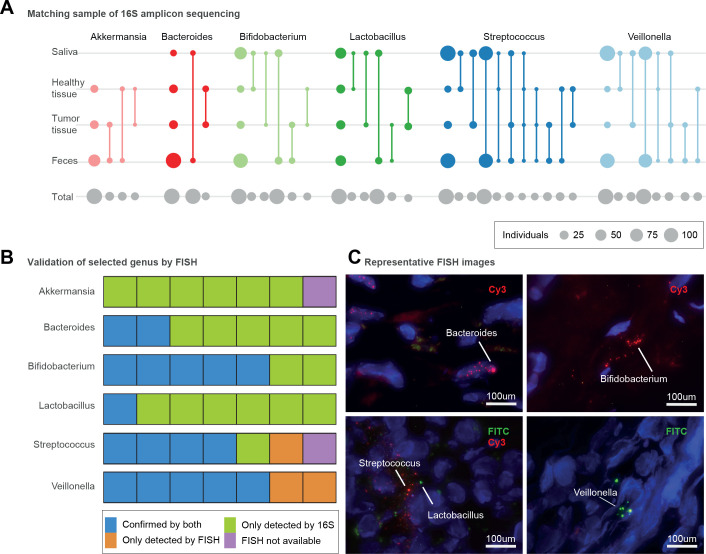
Results: Faecal metagenomic classifiers performed much better than saliva-based classifiers and identified patients with PDAC with an accuracy of up to 0.84 area under the receiver operating characteristic curve (AUROC) based on a set of 27 microbial species, with consistent accuracy across early and late disease stages. Performance further improved to up to 0.94 AUROC when we combined our microbiome-based predictions with serum levels of carbohydrate antigen (CA) 19-9, the only current non-invasive, Food and Drug Administration approved, low specificity PDAC diagnostic biomarker. Furthermore, a microbiota-based classification model confined to PDAC-enriched species was highly disease-specific when validated against 25 publicly available metagenomic study populations for various health conditions (n=5792). Both microbiome-based models had a high prediction accuracy on a German validation population (n=76). Several faecal PDAC marker species were detectable in pancreatic tumour and non-tumour tissue using 16S rRNA sequencing and fluorescence in situ hybridisation.
Conclusion: Taken together, our results indicate that non-invasive, robust and specific faecal microbiota-based screening for the early detection of PDAC is feasible.
Keywords: cancer prevention; intestinal microbiology; pancreatic cancer; pancreatic tumours; screening.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: EK, TSBS, JW, OMM, EM-M, GZ, LE, SR-P, FXR, NM and PB have a pending patent application (application number: EP21382876.7) for early detection of pancreatic cancer based on microbial biomarkers. The other authors declare no conflicts of interest.
Figures
Comment in
-
Finding clues in unexpected places: detection of pancreatic cancer through the faecal microbiome.Gut. 2022 Jul;71(7):1247-1248. doi: 10.1136/gutjnl-2021-326710. Epub 2022 Mar 8. Gut. 2022. PMID: 35260443 Free PMC article. No abstract available.
-
The microbiome as a potential diagnostic biomarker for pancreatic ductal adenocarcinoma (PDAC).Hepatobiliary Surg Nutr. 2022 Oct;11(5):752-754. doi: 10.21037/hbsn-22-380. Hepatobiliary Surg Nutr. 2022. PMID: 36268252 Free PMC article. No abstract available.
-
Gut microbiota as non-invasive diagnostic and prognostic biomarkers for natural killer/T-cell lymphoma.Gut. 2023 Oct;72(10):1999-2002. doi: 10.1136/gutjnl-2022-328256. Epub 2022 Nov 8. Gut. 2023. PMID: 36347595 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical