

Ethnic disparities in hospitalisation and hospital-outcomes during the second wave of COVID-19 infection in east London
- PMID: 35260620
- PMCID: PMC8904852
- DOI: 10.1038/s41598-022-07532-6
Ethnic disparities in hospitalisation and hospital-outcomes during the second wave of COVID-19 infection in east London
Abstract
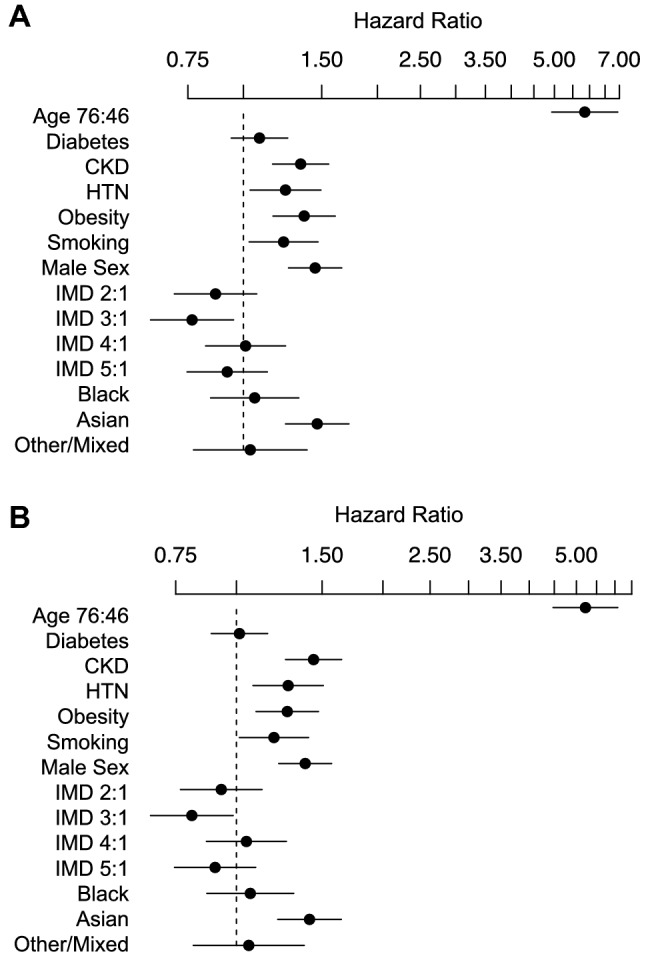
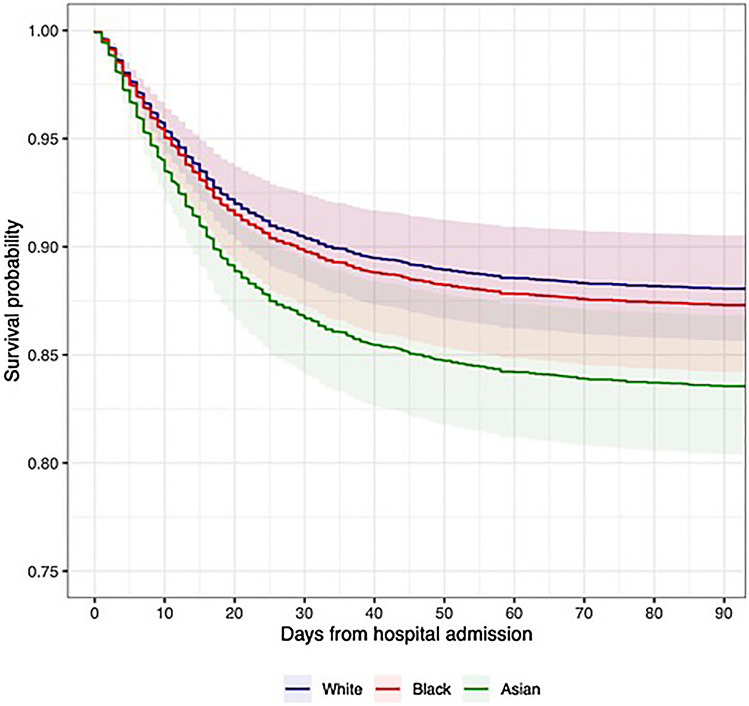
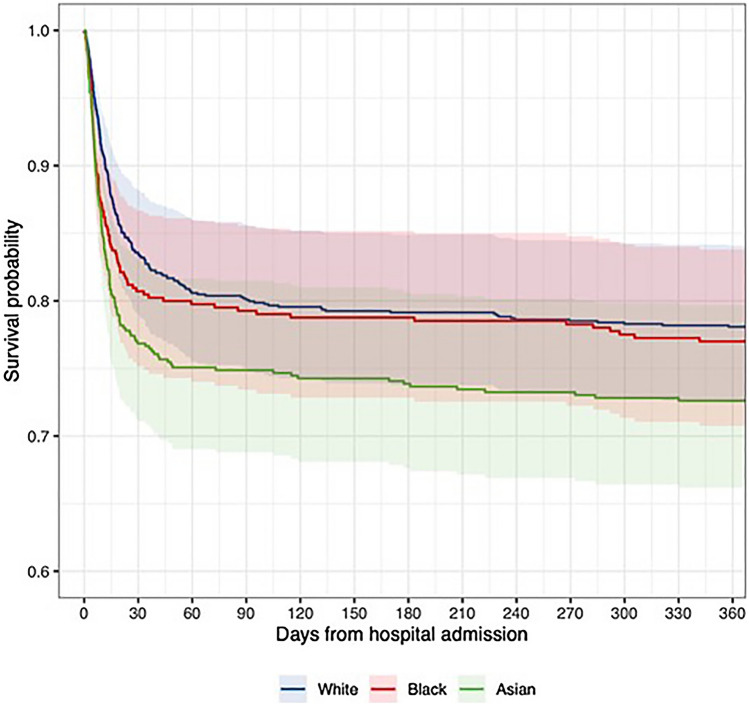
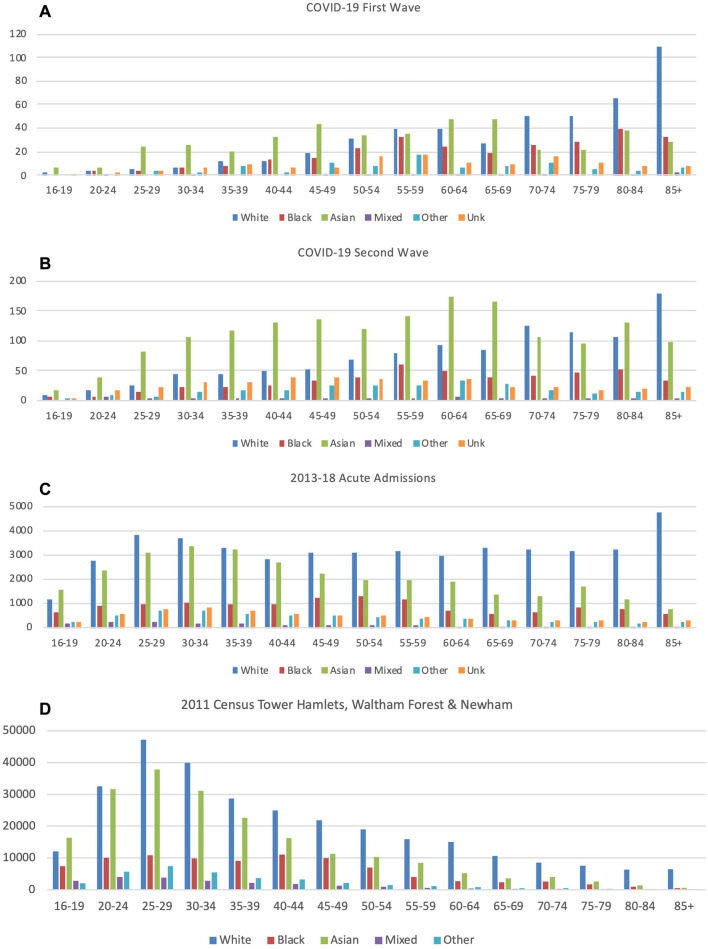
It is unclear if changes in public behaviours, developments in COVID-19 treatments, improved patient care, and directed policy initiatives have altered outcomes for minority ethnic groups in the second pandemic wave. This was a prospective analysis of patients aged ≥ 16 years having an emergency admission with SARS-CoV-2 infection between 01/09/2020 and 17/02/2021 to acute NHS hospitals in east London. Multivariable survival analysis was used to assess associations between ethnicity and mortality accounting for predefined risk factors. Age-standardised rates of hospital admission relative to the local population were compared between ethnic groups. Of 5533 patients, the ethnic distribution was White (n = 1805, 32.6%), Asian/Asian British (n = 1983, 35.8%), Black/Black British (n = 634, 11.4%), Mixed/Other (n = 433, 7.8%), and unknown (n = 678, 12.2%). Excluding 678 patients with missing data, 4855 were included in multivariable analysis. Relative to the White population, Asian and Black populations experienced 4.1 times (3.77-4.39) and 2.1 times (1.88-2.33) higher rates of age-standardised hospital admission. After adjustment for various patient risk factors including age, sex, and socioeconomic deprivation, Asian patients were at significantly higher risk of death within 30 days (HR 1.47 [1.24-1.73]). No association with increased risk of death in hospitalised patients was observed for Black or Mixed/Other ethnicity. Asian and Black ethnic groups continue to experience poor outcomes following COVID-19. Despite higher-than-expected rates of hospital admission, Black and Asian patients also experienced similar or greater risk of death in hospital since the start of the pandemic, implying a higher overall risk of COVID-19 associated death in these communities.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Raisi-Estabragh Z, et al. Greater risk of severe COVID-19 in Black, Asian and Minority Ethnic populations is not explained by cardiometabolic, socioeconomic or behavioural factors, or by 25(OH)-vitamin D status: study of 1326 cases from the UK Biobank. J. Public Health (Oxf) 2020;42:451–460. doi: 10.1093/pubmed/fdaa095. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
