

Cervical spine immobilization does not interfere with nasotracheal intubation performed using GlideScope videolaryngoscopy: a randomized equivalence trial
- PMID: 35260735
- PMCID: PMC8904815
- DOI: 10.1038/s41598-022-08035-0
Cervical spine immobilization does not interfere with nasotracheal intubation performed using GlideScope videolaryngoscopy: a randomized equivalence trial
Abstract
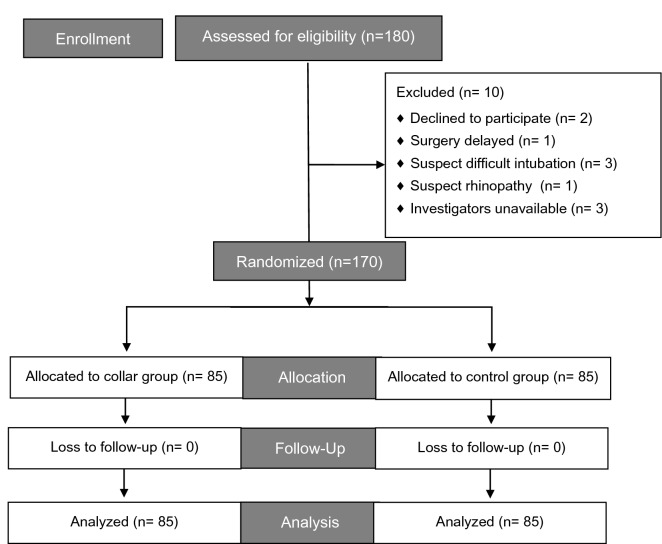
GlideScope-assisted nasotracheal intubation (NTI) has been proposed as an alternative to difficult orotracheal intubation for critical patients or those under cervical immobilization. We evaluated the difficulty of performing NTI using GlideScope under cervical orthosis. A total of 170 patients scheduled for elective cervical spinal surgery that required NTI were randomized to receive cervical immobilization using a cervical collar (collar group) or no cervical immobilization at all (control group) before anesthetic induction (group assignment at 1:1 ratio). All NTI during anesthetic induction were performed using the GlideScope. The primary outcome was time to intubation. The secondary outcomes were ease of intubation, including the necessity of auxiliary manipulations to assist intubation, and the nasotracheal intubation difficulty scale (nasoIDS). An exploratory analysis identified morphometric parameters as predictors of time to intubation, the necessity of auxiliary manipulations, and a nasoIDS score ≥ 4. For time to intubation, the mean difference (collar group-control) was - 4.19 s, with a 95% confidence interval (CI) of - 13.9 to 5.52 that lay within our defined equivalence margin of 16 s. Multivariate regressions precluded the association of cervical immobilization with a necessity for auxiliary manipulations (adjusted odds ratio [aOR] 0.53, 95% CI [0.26-1.09], P = 0.083) and a nasoIDS ≥ 4 (aOR 0.94 [0.84-1.05], P = 0.280). Among all morphometric parameters, the upper lip bite test class was predictive of a longer time to intubation (all analyses relative to class 1, 14 s longer for class 2, P = 0.032; 24 s longer for class 3, P = 0.070), increased necessity for auxiliary manipulation (aOR 2.29 [1.06-4.94], P = 0.036 for class 2; aOR 6.12 [1.04-39.94], P = 0.045 for class 3), and nasoIDS ≥ 4 (aOR 1.46 [1.14-1.89], P = 0.003 for class 3).The present study demonstrated that GlideScope achieved NTI in patients with or without cervical immobilization equivalently with respect to intubation time and ease.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
