

Lactate Clearance as a Surrogate for Mortality in Cardiogenic Shock: Insights From the DOREMI Trial
- PMID: 35261289
- PMCID: PMC9075306
- DOI: 10.1161/JAHA.121.023322
Lactate Clearance as a Surrogate for Mortality in Cardiogenic Shock: Insights From the DOREMI Trial
Abstract
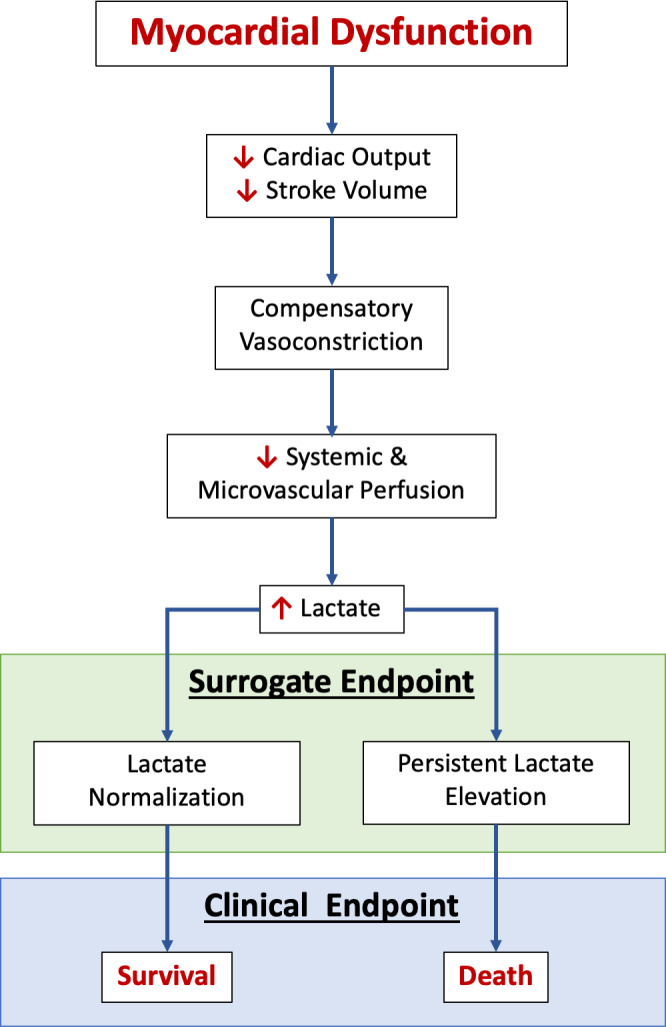
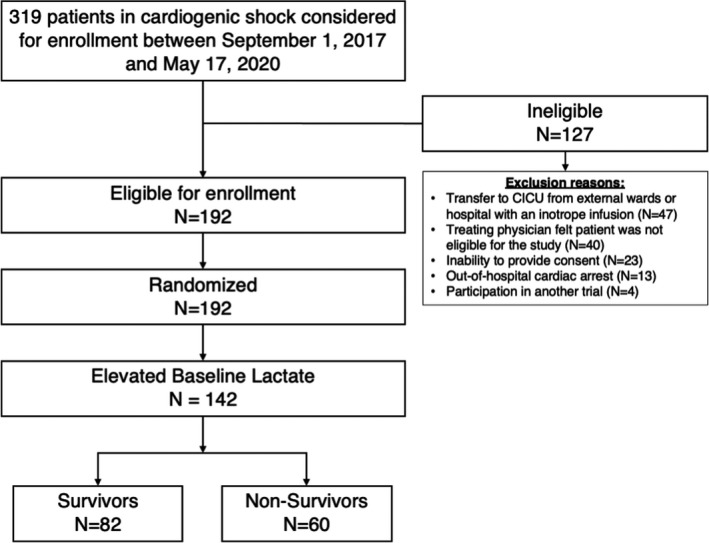
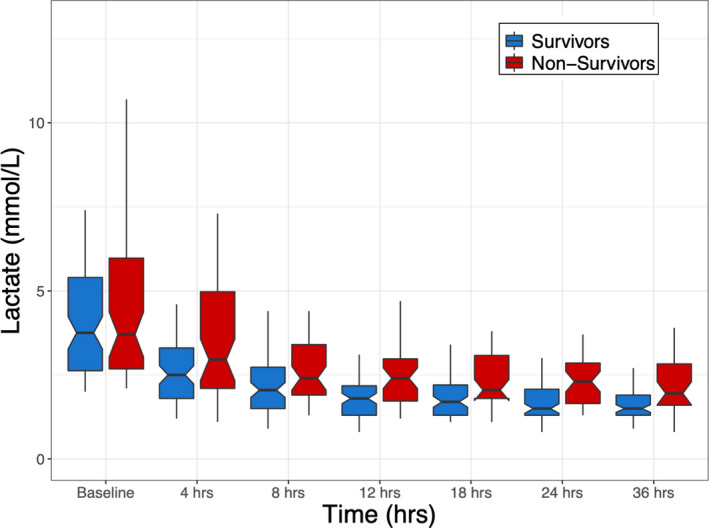
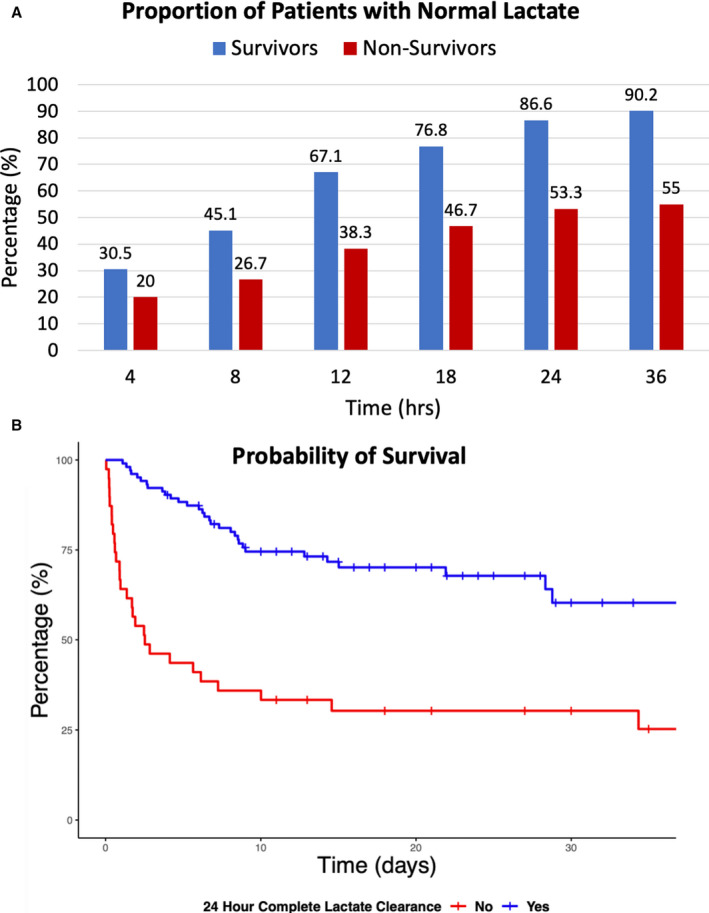
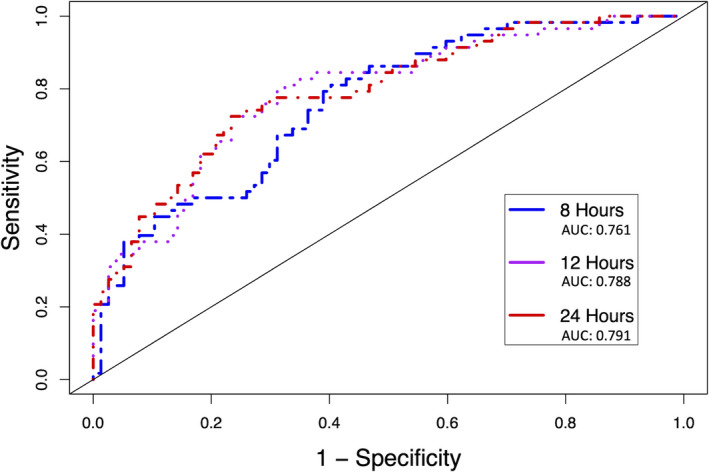
Background Recent studies have shown improved outcomes in cardiogenic shock through protocols directed toward early identification and initiation of mechanical circulatory support. However, objective therapeutic targets-based on clinical and/or laboratory data-to guide real-time clinical decision making are lacking. Lactate clearance has been suggested as a potential treatment target because of its independent association with mortality. Methods and Results In a post hoc analysis of the DOREMI (Dobutamine Compared to Milrinone in the Treatment of Cardiogenic Shock) trial-a randomized, double-blind, controlled trial comparing milrinone to dobutamine in the treatment of cardiogenic shock-we used prospectively collected lactate data to evaluate lactate clearance as a surrogate marker for in-hospital mortality. In total, 82 (57.7%) patients survived to hospital discharge (survivors). In multivariate logistic regression analysis, complete lactate clearance, percentage lactate clearance, and percentage lactate clearance per hour were independently associated with survival beginning as early as 8 hours after enrollment. Complete lactate clearance was the strongest predictor of survival at all time points, with odds ratios ranging between 2.46 (95% CI, 1.09-5.55; P=0.03) at 8 hours to 5.44 (95% CI, 2.14-13.8; P<0.01) at 24 hours. Conclusions Complete lactate clearance is a strong and independent predictor of in-hospital survival in patients with cardiogenic shock. Together with previously published data, these results further support the validity of lactate clearance as an appropriate surrogate for mortality and as a potential therapeutic target in future cardiogenic shock trials. Registration URL: https://www.clinicaltrials.gov; Unique identifier: NCT03207165.
Keywords: cardiogenic shock; lactate clearance; mortality; surrogate end point.
Figures
References
-
- Goldberg RJ, Makam RCP, Yarzebski J, McManus DD, Lessard D, Gore JM. Decade‐long trends (2001–2011) in the incidence and hospital death rates associated with the in‐hospital development of cardiogenic shock after acute myocardial infarction. Circ Cardiovasc Qual Outcomes. 2016;9:117–125. doi: 10.1161/CIRCOUTCOMES.115.002359 - DOI - PMC - PubMed
-
- van Diepen S, Katz JN, Albert NM, Henry TD, Jacobs AK, Kapur NK, Kilic A, Menon Venu, Ohman EM, Sweitzer NK, Thiele H, Washam JB, Cohen MG. American Heart Association Council on Clinical Cardiology; Council on Cardiovascular and Stroke Nursing; Council on Quality of Care and Outcomes Research; and Mission: Lifeline . Contemporary management of cardiogenic shock: a scientific statement from the American Heart Association. Circulation. 2017;136:e232–e268. doi:10.1161/CIR.0000000000000525 - DOI - PubMed
-
- Thayer KL, Zweck E, Ayouty M, Garan AR, Hernandez‐Montfort J, Mahr C, Morine KJ, Newman S, Jorde L, Haywood JL, et al. Invasive hemodynamic assessment and classification of in‐hospital mortality risk among patients with cardiogenic shock. Circ Heart Fail. 2020;13:e007099. doi: 10.1161/CIRCHEARTFAILURE.120.007099 - DOI - PMC - PubMed
-
- Kolte D, Khera S, Aronow WS, Mujib M, Palaniswamy C, Sule S, Jain D, Gotsis W, Ahmed A, Frishman WH, et al. Trends in incidence, management, and outcomes of cardiogenic shock complicating ST‐elevation myocardial infarction in the United States. J Am Heart Assoc. 2014;3:e000590. doi: 10.1161/JAHA.113.000590 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
