

Socioeconomic deprivation and survival outcomes in patients with colorectal cancer
- PMID: 35261805
- PMCID: PMC8899994
Socioeconomic deprivation and survival outcomes in patients with colorectal cancer
Abstract
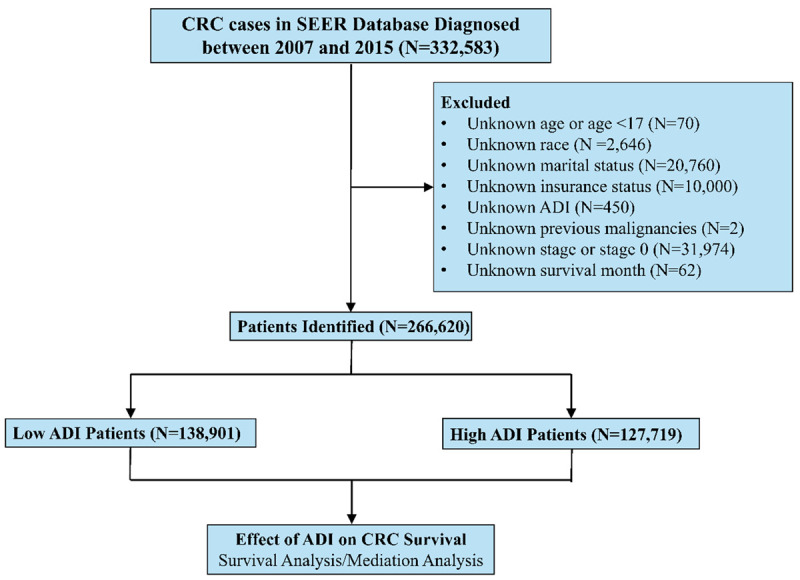
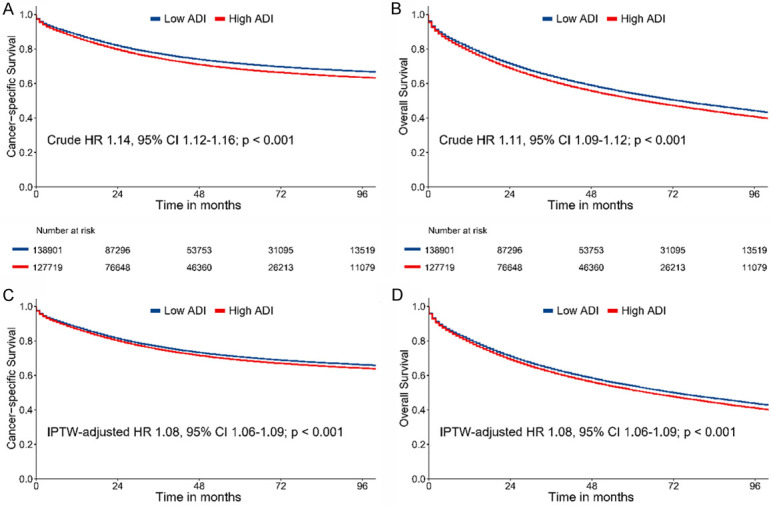
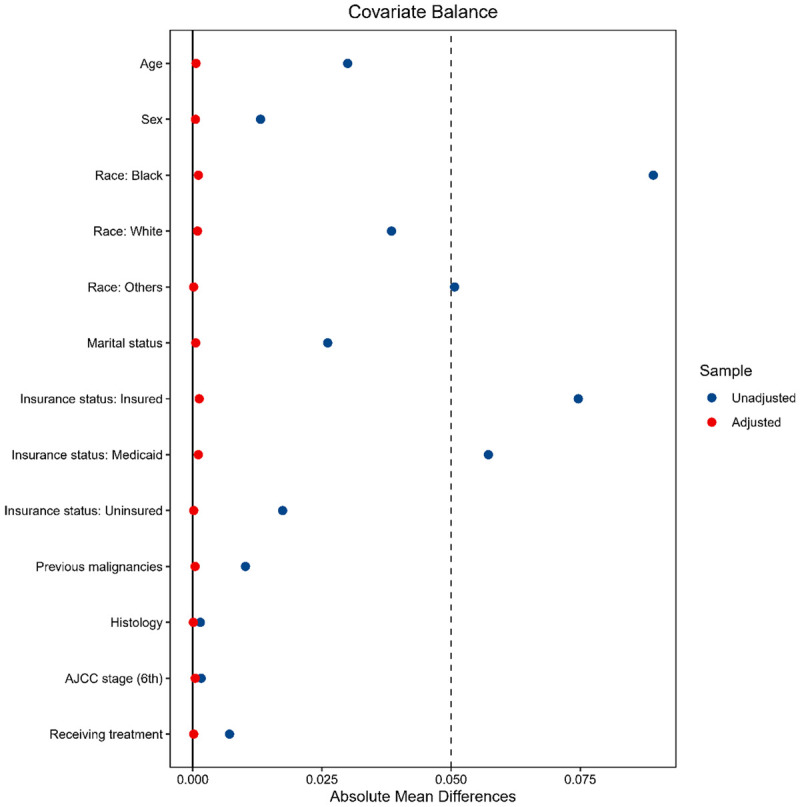
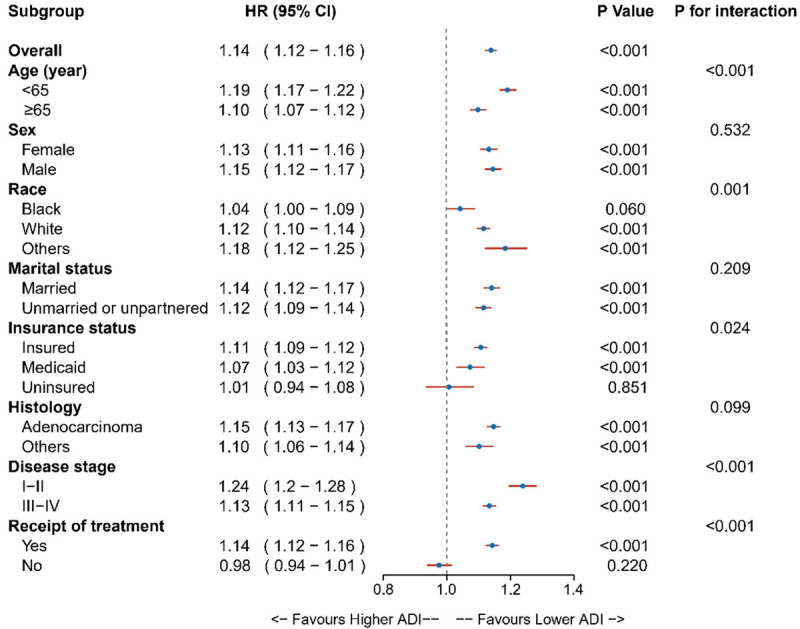
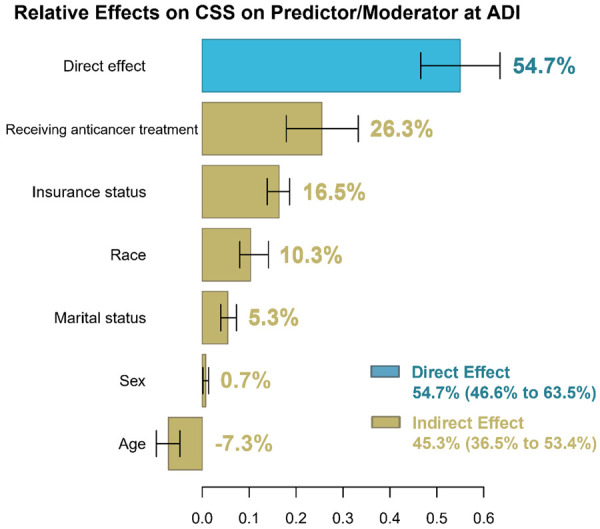
Socioeconomic deprivation has been linked to detrimental healthcare outcomes. We sought to examine whether patients with colorectal cancer (CRC) from socioeconomically disadvantaged areas experience worse survival outcomes and how it interacts with other factors. In this population-based study, patients with CRC diagnosed between 2007 to 2015 in the SEER program were reviewed. Socioeconomic deprivation was measured using the Area Deprivation Index (ADI) linked to patients' residence addresses. The effect of ADI on cancer-specific survival and overall survival was evaluated using survival analysis. The Inverse Probability of Weighted (IPW) method and multiple regression was performed to account for the confounding bias. Subgroup analyses were used to test interactions. Multiple mediation analysis was used to estimate the mediating effects. Overall, 266,620 eligible patients were included in further analyses. Compared with low ADI patients, high ADI patients had more unfavorable characteristics and worse cancer-specific (hazard ratio [HR] 1.14, 95% CI 1.12-1.16, P<.001) and overall survival (HR 1.11, 95% CI 1.09-1.12, P<0.001). The results were similar after accounting for confounding factors using the IPW and multiple regression methods. Subgroup analyses revealed the relative robustness of ADI as a prognostic factor. They detected significant interactions between ADI and other covariates on cancer survival, such as age, race, insurance status, disease stage, and receipt of treatment. Multiple mediation analyses identified several factors mediating survival disparities, including anticancer therapy, insurance status, race, marital status, and age. This study suggested that high ADI CRC patients were associated with more unfavorable characteristics at presentation and lower cancer and noncancer survival after treatment than their low ADI counterparts. Multiple factors interacted and mediated these survival disparities associated with the ADI.
Keywords: SEER program; Socioeconomic deprivation; area deprivation index; cancer survival; colorectal cancer; neighbourhood disadvantage.
AJCR Copyright © 2022.
Conflict of interest statement
None.
Figures
References
-
- Siegel R, Miller K, Fuchs H, Jemal A. Cancer statistics, 2021. CA Cancer J Clin. 2021;71:7–33. - PubMed
-
- Siegel R, Miller K, Goding Sauer A, Fedewa S, Butterly L, Anderson J, Cercek A, Smith R, Jemal A. Colorectal cancer statistics, 2020. CA Cancer J Clin. 2020;70:145–164. - PubMed
-
- Lin J, Perdue L, Henrikson N, Bean S, Blasi P. Screening for colorectal cancer: updated evidence report and systematic review for the US Preventive Services Task Force. JAMA. 2021;325:1978–1998. - PubMed
-
- Patel A, Gantz O, Zagadailov P, Merchant AM. The role of socioeconomic disparity in colorectal cancer stage at presentation. Updates Surg. 2019;71:523–531. - PubMed
LinkOut - more resources
Full Text Sources