

Association of Physician Referrals with Timely Cancer Care Using Tumor Registry and Claims Data
- PMID: 35261937
- PMCID: PMC8896170
- DOI: 10.1089/heq.2021.0089
Association of Physician Referrals with Timely Cancer Care Using Tumor Registry and Claims Data
Abstract
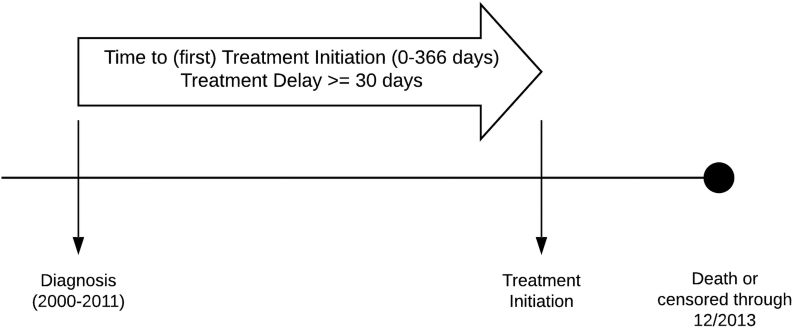
More Americans are being screened for and more are surviving colorectal cancer due to advanced treatments and better quality of care; however, these benefits are not equitably distributed among diverse or older populations. Differential care delivery outcomes are driven by multiple factors, including access to timely treatment that comes from high-quality care coordination. Providers help ensure such coordinated care, which includes timely referrals to specialists. Variation in referrals between providers can also result in differences in treatment plans and outcomes. Patients who are more often referred between the same diagnosing and treating providers may benefit from more timely care compared to those who are not. Our objective is to examine patterns of referral, or patient-sharing networks (PSNs), and our outcome, treatment delay of 30-days (yes/no). We hypothesize that if a patient is in a PSN they will have lower odds of a 30-day treatment initiation delay. Our observational population-based analysis using the National Cancer Institute (NCI)-linked tumor registry and Medicare claims database includes records for 27,689 patients diagnosed with colorectal cancer from 2001 to 2013, and treated with either chemotherapy, radiotherapy, or surgery. We modeled the adjusted odds of a delay and found 17.04% of patients experienced a 30-day delay in initial treatment. Factors that increased odds of a delay were lack of membership in a PSN (adjusted odds ratio [AOR]: 2.20; 95% confidence interval [CI]: 1.71-2.84), racial/ethnic minority status, and having multiple comorbidities. Provider characteristics significantly associated with greater odds of a delay were if dyads were not in the same facility (AOR: 1.95; 95% CI: 1.81-2.10), if providers were different genders, most notably male (diagnosing) and female (treating) [AOR: 1.23; 95% CI: 1.08-1.40, p = 0.0015]. PSNs appear to be associated with reduced of a care delay. The associations observed in our study address the demand for developing multilevel interventions to improve the delivery and coordination of high-quality of care for older cancer patients.
Keywords: cancer and aging; communication; health care delivery; health disparities; patient–provider communication; systems science.
© Melody K. Schiaffino et al., 2022; Published by Mary Ann Liebert, Inc.
Conflict of interest statement
No competing financial interests exist.
Figures


Similar articles
-
Surgeon and Care Team Network Measures and Timely Breast Cancer Treatment.JAMA Netw Open. 2024 Aug 1;7(8):e2427451. doi: 10.1001/jamanetworkopen.2024.27451. JAMA Netw Open. 2024. PMID: 39207756 Free PMC article.
-
Genetic counseling practices among outpatient obstetric providers in the Northeast.Am J Obstet Gynecol MFM. 2023 Nov;5(11):101150. doi: 10.1016/j.ajogmf.2023.101150. Epub 2023 Sep 6. Am J Obstet Gynecol MFM. 2023. PMID: 37683764
-
Racial and ethnic differences in perception of provider cultural competence among patients with depression and anxiety symptoms: a retrospective, population-based, cross-sectional analysis.Lancet Psychiatry. 2021 Nov;8(11):957-968. doi: 10.1016/S2215-0366(21)00285-6. Epub 2021 Sep 23. Lancet Psychiatry. 2021. PMID: 34563316 Free PMC article.
-
[Patient-sharing networks : New approaches in the analysis and transformation of geographic variation in healthcare].Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2017 Dec;60(12):1356-1371. doi: 10.1007/s00103-017-2641-7. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2017. PMID: 29064035 Review. German.
-
Increasing Access: Reducing Referral Delay in Patients With Ambulatory Advanced HF.J Card Fail. 2025 Mar 25:S1071-9164(25)00159-9. doi: 10.1016/j.cardfail.2025.03.015. Online ahead of print. J Card Fail. 2025. PMID: 40147585 Review.
Cited by
-
Surgeon and Care Team Network Measures and Timely Breast Cancer Treatment.JAMA Netw Open. 2024 Aug 1;7(8):e2427451. doi: 10.1001/jamanetworkopen.2024.27451. JAMA Netw Open. 2024. PMID: 39207756 Free PMC article.
-
The Colocation Model in Community Cancer Care: A Description of Patient Clinical and Demographic Attributes and Referral Pathways.JCO Oncol Pract. 2023 Jun;19(6):e916-e926. doi: 10.1200/OP.22.00487. Epub 2023 Mar 20. JCO Oncol Pract. 2023. PMID: 36940391 Free PMC article. Review.
-
A Scoping Review of Multilevel Patient-Sharing Network Measures in Health Services Research.Med Care Res Rev. 2025 Jun;82(3):203-224. doi: 10.1177/10775587241304140. Epub 2024 Dec 30. Med Care Res Rev. 2025. PMID: 40271968 Free PMC article.
-
Within-Physician Differences in Patient Sharing Between Primary Care Physicians and Cardiologists Who Treat White and Black Patients With Heart Disease.J Am Heart Assoc. 2023 Nov 21;12(22):e030653. doi: 10.1161/JAHA.123.030653. Epub 2023 Nov 20. J Am Heart Assoc. 2023. PMID: 37982233 Free PMC article.
References
-
- SEER. Cancer Stat Facts: Colorectal Cancer. Available at https://seer.cancer.gov/statfacts/html/colorect.html Accessed September 15, 2021.
-
- Asan O, Nattinger AB, Gurses AP, et al. . Oncologists' views regarding the role of electronic health records in care coordination. JCO Clin Cancer Inform. 2018;2:1–12. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources